





Abstract
An 82-year-old woman without any previous medical history arrived in the emergency department with severe pain in the entire abdomen since 5 h. Blood tests showed, apart from a CRP of 28 mg/l, no abnormalities. We decided to perform an abdominal ultrasound, which showed an easily compressible gallbladder, containing a small, mobile gallstone and free fluid in the abdomen. During ultrasound-guided punction of this fluid, bile is aspirated. We performed laparoscopy and confirmed a large amount of intraperitoneal bile. Upon inspecting the gallbladder a perforation is seen in the anti-hepatic side of the gallbladder. After performing a cholecystectomy, we opened the gallbladder and detected a dissection-like lesion, which provided access to the peritoneal cavity. The confirmed diagnosis was acute onset free perforation of the gallbladder. The perforation was probably caused by the small obstructing gallstone seen on ultrasound or by another small stone, which could not be visualized.
INTRODUCTION
Patients who suffer from acute abdominal pain often visit the emergency department for medical evaluation. A wide variety of diagnoses is seen and include those of vascular, visceral or infectious origin. In this study, we describe a very rare case of acute abdominal pain that is nonetheless relevant for any clinician who works in the surgical field.
CASE REPORT
An 82-year-old woman without any known medical comorbidity arrived in the emergency department early in the morning with extreme pain in the entire abdomen since 5 h. The pain had an acute onset, was severe and persisted throughout the night. The general practitioner on call has given her scopolaminebutyl, diclofenac and later morphine because of the severity of the pain. During physical examination we saw a painful, afebrile woman, with a diffusely tender abdomen and aggravation of the pain on palpation of the right lower quadrant. Blood tests show, apart from a CRP of 28 mg/l, no abnormalities. Gallstone colic, acute pancreatitis, stomach perforation and appendicitis are considered as plausible diagnoses at this point. We decided to perform an abdominal ultrasound, which shows an easily compressible gallbladder, containing a small, mobile gallstone (Fig. 1A and B), and free fluid in the abdomen (Fig. 1C). During ultrasound-guided punction of this intraperitoneal liquid, bile is aspirated (Fig. 1D). We performed a laparoscopy and confirmed a large amount of intraperitoneal bile. Upon inspecting the gallbladder, a perforation is seen in the anti-hepatic side of the gallbladder. After performing a laparoscopic cholecystectomy, we opened the gallbladder and detected a dissection-like lesion, which provided access to the peritoneal cavity (E and F). The gallstone that was seen during ultrasound could not be found and the cystic duct seems free of stones. Microscopy revealed a chronic cholecystitis (despite the absence of symptoms) with focally degenerative mucous membrane located around the perforation. The postoperative phase was uncomplicated. It seems that an acute hydropic state of the gallbladder, caused by a small obstructing bile stone, lead to a free perforation of the gallbladder and biliary peritonitis.
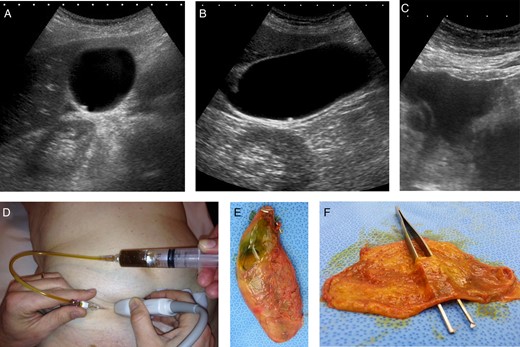
(A–F) Ultrasound shows an easily compressible, non-hydropic gallbladder and a small, mobile stone at the bottom of the gallbladder (A and B). In the right lower quadrant of the abdomen, free fluid is visible (C). Punction and aspiration of the fluid confirms that the free fluid is bile (D). During laparoscopy, a leaking gallbladder is seen, after cholecystectomy and opening of the gallbladder a perforation is confirmed (E and F).
DISCUSSION
Perforation of the gallbladder is one of the rare but severe complications of acute calculous cholecystitis, like empyema, gallstone ileus, cholecystoenteric fistula and emphysematous cholecystits [1]. Perforation of the gallbladder can occur as early as 24 h after the onset of acute cholecystitis, or after a few days to weeks [2]. According to different studies, an incidence rate of 3.3–5.9% is reported of acute and chronic perforations [1, 3]. In 1934, Niemeier described three types of free gallbladder perforations: Type 1 (acute) is associated with generalized biliary peritonitis. Type 2 (subacute) is recognized by local fluid at the site of the perforation and Type 3 is a chronic perforation associated with internal fistulas [4]. Our patient had a Type 1 perforation combined with a chronic cholecystitis, given the acute onset and the evident intraperitoneal bile. The perforation was probably caused by the small obstructing gallstone seen on ultrasound or by another small stone, which could not be visualized. Understandably, the diagnosis of an acute perforation in cholecystitis and immediate surgical intervention are very important in decreasing morbidity and mortality associated with this condition [5]. The case that we described seems very rare, since a perforation was found only several hours after the symptoms had started. Moreover, this patient had never experienced any serious abdominal pain, which does not correspond with the microscopy report. Despite the rareness of this case, we believe that it shows an important and possibly dangerous condition that needs to be considered in patients who visit the emergency department with acute abdominal pain.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}