





Abstract
Laparoscopic distal pancreatectomies became more common in the past few years as a safe and effective treatment option for benign and low-grade malignant tumors of the body and tail of the pancreas. Adequate exposure and wide operative field are crucial to perform this procedure, and this is achieved by retraction of the stomach with an angled liver retractor or a grasper through a subxiphoid trocar, that is usually used only to this purpose. We developed an innovative technique to retract the stomach during laparoscopic distal pancreatectomies that provides excellent operative field and frees the subxiphoid trocar to be used in other tasks during the surgery.
INTRODUCTION
In the past few years, there was a great increase in the diagnosis of benign tumors and low-grade malignancies of the pancreas, especially in young female individuals. This led to an increased demand for pancreatic resections that preserve healthy parenchyma and minimize surgical wounds, and laparoscopic distal pancreatectomy is an efficient technique to achieve those goals [1].
The first laparoscopic intervention on the pancreas was described by Bernheim in 1911. He performed a laparoscopic staging of a pancreatic cancer [2]. This procedure was only reintroduced by Cuscheri in 1978 [3]. Nevertheless, the first laparoscopic distal pancreatectomy was performed by Soper in 1994 on a pig, while the experience on humans began in 1996 with Gagner [4, 5].
Especially during laparoscopic procedures, adequate exposure and wide operative field are crucial [6]. In pancreatic laparoscopic procedures, the stomach must be efficiently retracted in order to obtain good working space.
During distal pancreatectomies, a subxiphoid trocar is placed exclusively to perform gastric retraction with an angled liver retractor that must be frequently repositioned to expose different parts of the pancreas or the spleen (when splenectomy associated). Other instruments may be used, but their use commonly results in damage to the stomach.
OPERATIVE TECHNIQUE
We developed a simple and fast technique that uses only a surgical polyester tape that enables effective and stable gastric retraction and frees the subxiphoid trocar to be in other tasks during the surgery, not only gastric retraction.
We used four trocars as follows (Fig. 1):
Subxiphoid 5 mm trocar
Transumbilical 10 mm trocar
Left anterior axillary 12 mm trocar
Right mid-clavicular 5 mm trocar
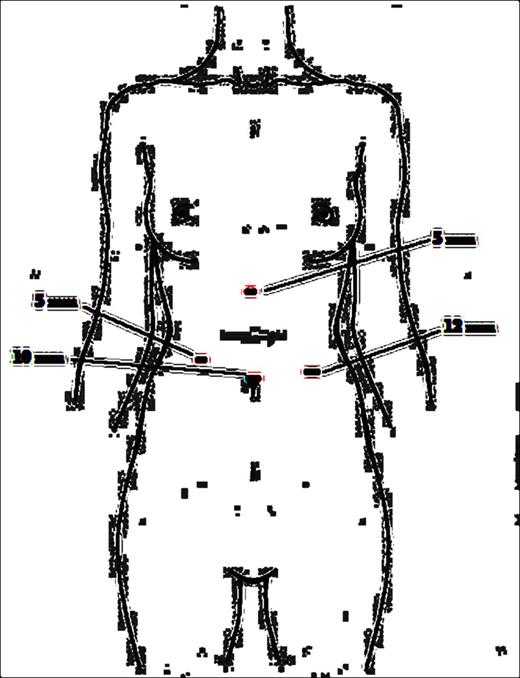
Trocar displacement.
First, we opened the great omentum from the antrum to the body, gaining access to the retroperitoneal space. Then, a small opening was performed on the lesser omentum, close to the antrum. A folded polyester cardiac tape was passed behind the stomach and pulled through the role on the lesser omentum. Then, the two ends of the tape are passed through the loop that was pulled through the opening on the lesser omentum (Fig. 2).
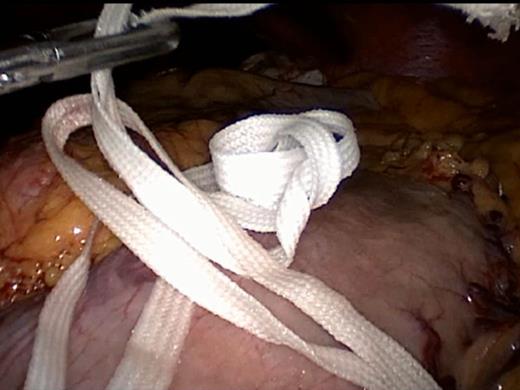
Passing the polyester tape around the stomach.
The two ends of the tape are then pulled outside the abdomen, though the subxiphoid trocar and the trocar is removed. After that, the trocar is put back in place leaving the two ends of the tape outside the trocar. This trocar can now be used by an assistant to help the surgeon in different tasks (Fig. 3).

Subxiphoid trocar back in place with a working instrument.
This maneuver allowed good operative view of the body of the pancreas and tumor (Fig. 4).
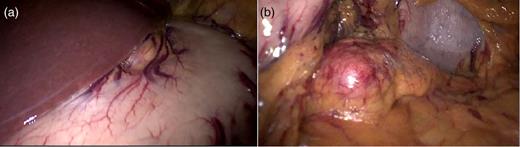
(a) Operative view on the beginning of the procedure and (b) operative view after gastric retraction with the polyester tape.
DISCUSSION
Laparoscopy distal pancreatectomy is a feasible and safe procedure that has several advantages to the open approach such as smaller incisions, reduced blood loss, time to first oral intake, lower complication rates and hospital stay [1, 7]. Moreover, most of the tumors of the body and tail of the pancreas are benign or low-grade malignancies incidentally diagnosed during routine ultra-sonographies on young females [7]. As a result, the laparoscopic approach to distal pancreatectomies is becoming increasingly popular, and it can be recommended as the treatment of choice for noninvasive and benign lesions [8].
Laparoscopic distal pancreatectomies are usually performed with four trocars. The camera is placed through a transumbilical trocar, and the instruments are placed through a right mid-clavicular trocar, a left anterior axillary trocar and a subxiphoid trocar, used by an assistant for gastric retraction (Fig. 1).
As the pancreas is a retroperitoneal organ that lies behind the stomach, the lesser sac must be reached by transecting the gastrocolic ligament. After that, both the stomach and the left lobe of the liver must be retracted upward in order to obtain adequate operative field and visualization of the neck, body and tail of the pancreas. This is usually achieved by applying upward traction to the stomach with a toothed grasper or an atraumatic flexible liver retractor through the subxiphoid trocar.
However, this may not be an easy task. As a result of limited haptic feedback and the loss of 3D visualization, excessive force may be applied to anatomic structures during retraction, resulting in the damage to the tissues [9]. Moreover, retractors may inadvertently move during important steps of the surgery as a result of the limited field of view provided by laparoscopes that precludes constant visualization of the retractors. To overcome these problems, different instruments have been designed to provide a stable platform to hold retractors [10].
Gastric retraction with the polyester tape through the subxiphoid trocar incision is an atraumatic maneuver that provides wide operative field and stable exposure of the pancreas.
One immediate result was to allow the assistant to perform other tasks during the procedure, such as suspending the pancreas while it is being mobilized out of the retroperitoneum and retraction the inferior pole of the spleen, converting the subxiphoid trocar into a two-simultaneous task port. This made some maneuvers easier to accomplish (Fig. 5).
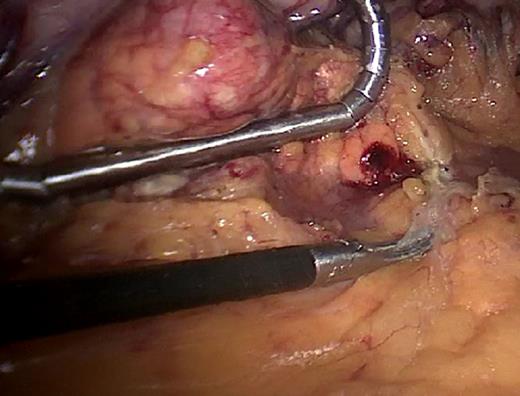
Assistant retracting the pancreas through the subxiphoid trocar.
Another advantage of the tape retraction of the stomach is that, when compared with articulating instrument holders, the polyester tape is a much cheaper and available product.
Gastric retraction with a polyester tape during laparoscopic distal pancreatectomy is a cheap, easy, atraumatic and effective maneuver. It provided adequate pancreatic exposure and wide operative field. It allowed the assistant to help the surgeon during different steps of the procedure, not only retracting the stomach, thus making the 5-mm subxiphoid port a multi-task access.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}