





Abstract
Elbow fractures are not uncommon in children, and some are associated with neurovascular injuries. Having a nerve injury in an elbow fracture without dislocation is rare and was not described in the literature. Here, we have reported probably the first case of an ulnar nerve injury in an elbow fracture without dislocation. A 9-year-old female presented to the emergency department after falling off a monkey bar. She had a painful, swollen and tender right elbow with no history or clinical signs of an elbow dislocation but had complete ulnar nerve palsy. She was managed initially with analgesia and plaster application and was taken directly to the operating theatre. Examination under anaesthesia revealed no elbow joint instability. The ulnar nerve was found entrapped between the trochlea and proximal ulna, intra-articularly. The medial epicondyle was also found avulsed from the humerus, with an incarcerated medial epicondylar fragment in the elbow joint.
INTRODUCTION
Elbow fractures are among the most common traumatic injuries in the paediatric population, consisting of ∼15% of all paediatric fractures [1, 2]. Humeral medial epicondyle fractures, in the paediatric population, account for up to 20% of elbow fractures, 60% of which are associated with an elbow dislocation [3]. The chance of median and ulnar nerve injuries, an incarcerated fragment in the joint, as well as other complications, further increases when a fracture is associated with a dislocation.
We present the case of a child who sustained a medial epicondyle fracture of the elbow, with a complete ulnar nerve palsy but without a joint dislocation, who was found intraoperatively to have ulnar nerve entrapment in the ulnohumeral joint. The rare occurrence of complications relating to both acute and late ulnar nerve entrapments have been reported before in literature—including following supracondylar fractures, medial epicondyle fractures with elbow dislocations, forearm fractures and Galeazzi fracture dislocations. However, there have been no reports describing an ulnar nerve intra-articular entrapment, with a medial epicondyle fracture but without an elbow dislocation.
CASE REPORT
A 9-year-old girl presented to the emergency department with right elbow pain and swelling, after falling from a monkey bar onto her right elbow. She had no previous history of elbow or ulnar nerve problems. On examination, her right elbow was swollen, tender with limited movements. She had no history or clinical signs of an elbow dislocation, but she had a complete ulnar nerve palsy [with the absence of sensation and increased 2-point discrimination, Medical Research Council (MRC) sensation grading S0; MRC power grading 0/5 of intrinsic muscles of the hand, the little finger flexor digitorum profundus (FDP) and flexor carpi ulnaris (FCU); Froment's sign was positive), but there was no evidence of vascular compromise. A plain radiograph showed that the medial epicondylar apophysis had been avulsed into the ulna humeral joint space, but there was no other fracture or dislocation seen (Fig. 1A and B).

Plain radiographs of the injured right elbow: (A) anteroposterior view and (B) lateral view. Arrows highlight the avulsed medial epicondyle.
She was taken directly to the operating theatre for emergency surgery, and an examination under anaesthesia revealed no elbow joint instability. The elbow was approached through a routine medial incision. The ulnar nerve was not found in the anatomical position, so further exploration was undertaken. The ulnar nerve was subsequently found to be trapped between the trochlea and proximal ulna, intra-articularly (Fig. 2). The nerve was severely bruised but in continuity. The medial epicondyle was also found avulsed from the humerus, with an incarcerated medial epicondylar fragment in the elbow joint. The nerve was transposed into the anatomical position after complete decompression was performed. The medial epicondyle was reduced to its anatomical position and fixed with a single cortical screw. A plaster was applied at 90° of elbow flexion.
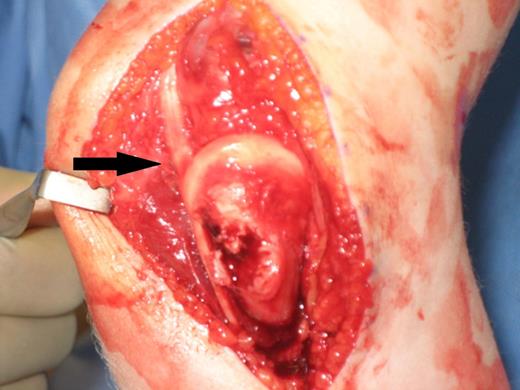
Intraoperative image showing the intra-articular entrapment of the ulnar nerve highlighted by the arrow.
A few hours post-operatively the sensation over the ulnar territory started to improve (MRC grading S2), FCU and FDP had partially recovered (power improving to MRC grading 3/5), but there was still MRC grading 1/5 of the intrinsic muscles of the hand.
On the first post-operative day, the patient's sensation over the ulnar territory was still reduced. The FCU and FDP were fully recovered with a MRC grading of 5/5, but the intrinsic muscles of the hand remained weak.
At 2 weeks follow-up, the wound had healed well and the plaster was changed to an above elbow cylinder cast. Repeat plain radiographs were satisfactory. Neurological examination of her hand revealed some still reduced sensation over the ulnar nerve territory, normal FCU and FDP function, with some further recovery of the intrinsic muscles of the hand (MRC grading 3/5).
At 5 weeks follow-up, the plaster cast was removed and the patient had a good range of motion of the elbow, with no signs of instability. She had a MRC grading of 5/5 of all the muscles, including the intrinsic muscles of the hand, and Froment's sign was negative, but there was still some reduced sensation (MRC grading S3). Physiotherapy was initiated.
At 5 months follow-up, the patient had full range of movement of the stable elbow with completely recovered ulna nerve function. The plain radiographs confirmed that the fracture healed (Fig. 3A and B).

Plain radiographs showing the healed fracture of the right elbow at 5 months: (A) anteroposterior view and (B) lateral view.
DISCUSSION
Elbow fractures are one of the most common injuries in children. Neurovascular injuries are not uncommon in fractures associated with a dislocation.
The contribution of the soft tissue structures around the elbow is of great importance in the stabilization of the elbow. Knowledge of the anatomy and biomechanics of the elbow, particularly the soft tissue and bony constraints, is of paramount importance in the diagnosis, management and long-term sequelae of injuries [4]. In children, as the bony constraints of the elbow are not well developed, the stability of the elbow depends mainly on the soft tissue structures. Therefore, elbow dislocations in children will result in signs of damage of the soft tissue structures of the elbow.
Treatment of medial epicondyle fractures is controversial. However, open reduction with internal fixation of the epicondyle fragment is clearly indicated in cases of intra-articular entrapment of the fragment, on suspicion of entrapment of the ulnar nerve, or in cases of marked instability of the elbow [5].
A medial epicondyle fracture associated with elbow dislocation, in children, may not be easily diagnosed on conventional radiographs because of the small size of the fragment, its ‘hidden’ position behind the distal humerus and the fact that it can be mistaken for the trochlear ossification centre [5].
In the case presented, complete ulnar nerve palsy was present without any evidence of elbow dislocation in the history and with there being no signs of elbow instability intra-operatively. Prompt clinical assessment and surgical treatment confirmed the intra-articular ulna nerve position and avoided that a simple reversible neurapraxia further developed into an irreversible devastating nerve lesion.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}