





Abstract
Since the term odontogenic keratocyst first appeared in the literature, controversy has surrounded its terminology and surgical management. Recent articles would suggest that surgical opinion is still divided between aggressive radical resection and a more conservative approach. We present an interesting case of a large keratocystic odontogenic tumour shown to have eroded through bony cortices and present within soft tissues that was satisfactorily managed conservatively by decompression and secondary enucleation.
INTRODUCTION
The term odontogenic keratocyst as a distinct entity was first described by Philipsen [1], who used the term to describe jaw cysts exhibiting keratinization of their epithelial linings. Lesions present most frequently in the second, third and fourth decades of life. Predilection for male gender has been reported with a male-to-female ratio of 2:1 [2]. It is one of the most controversial pathological entities. The World Health Organization recent classification of head and neck tumours reclassified the keratocyst as a benign neoplasm recommending the term keratocystic odontogenic tumour (KCOT) [3]. The recurrence rates are variable depending on the type of treatment. One recent systematic analysis of the recurrence rates showed that it was 0% for resection, 0% for enucleation with peripheral ostectomy and Carnoy's solution, 18.18% for enucleation with peripheral ostectomy, 26.09% for enucleation alone, 40% for marsupialization and 50% for enucleation with Carnoy's solution. The overall recurrence rate was 23.15% [4]. Due to this, usually a more aggressive approach is taken while treating KCOT.
CASE REPORT
A 25-year-old man presented with a 2-month history of facial pain and limited mouth opening associated with a 3-week history of swelling of the right cheek. Radiographic analysis revealed a loculated, fluid-filled, well-demarcated lesion destroying and expanding the ascending ramus, extending out into the soft tissues, from the condyle down to the angle (Fig. 1).
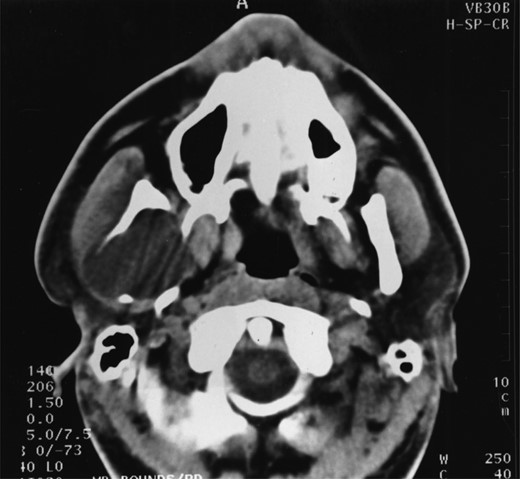
A well-demarcated lesion extending out into the soft tissues from the ramus of the mandible.
Incisional biopsy and histological examination revealed KCOT.
A decision was made to decompress the lesion to try and shrink the cystic space, encouraging bony infill. Over the following 3 months the patient underwent a further three re-packing procedures with irrigation of the cavity. The site of the cyst and difficulty of access necessitated general anaesthesia. The patient was admitted on one occasion for intra-venous antibiotics following an acute infective episode affecting the area. During the third operative procedure a split nasopharyngeal tube was inserted into the cyst cavity and sutured in position (Fig. 2). The patient was encouraged to flush the cavity clean through the tube drain.
A nasopharyngeal tube in position.
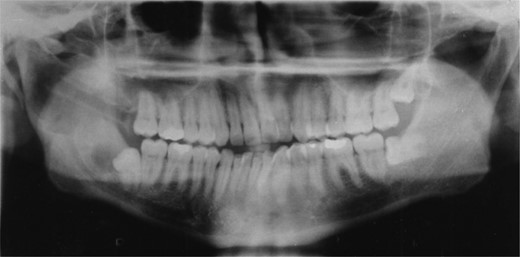
Radiographic examination over the following few months showed new bone formation and within 9 months of the initial biopsy the drain was expelled by formation of new bone (Fig. 3). One year after the commencement of treatment the patient was admitted for enucleation of the cystic remnant. At the time of this procedure a small cyst was removed from the right upper ramus and condylar neck, together, with a separate cyst associated with the lower right wisdom tooth. The patient made an uneventful post-operative recovery and histology revealed two KCOTs with a thick parakeratinized type of epithelium typical of radicular cysts.
Demonstrates bony infill with the nasopharyngeal tube in place.
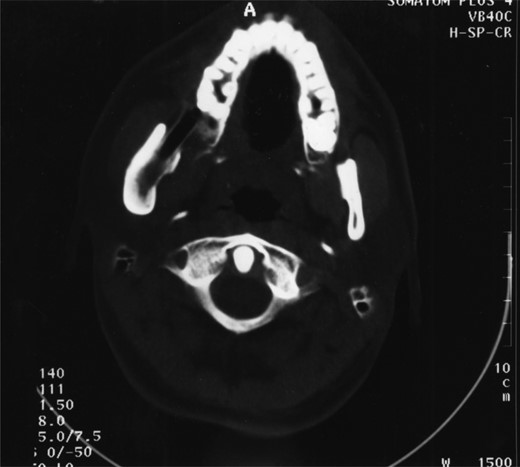
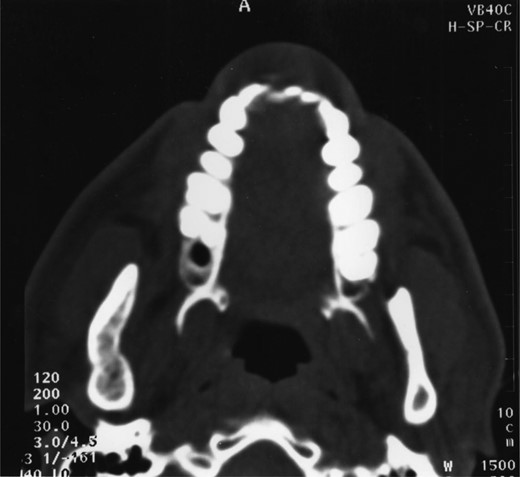
Plain films along with CT scan, with 3 mm slices, were performed a further year later and showed good bone regeneration in the right ramus and condylar neck (Figs 4 and 5). No evidence of cystic recurrence was seen and no abnormalities within the adjacent soft tissues. High-resolution magnetic resonance imaging also confirmed the absence of cystic remnants. The patient has now been reviewed for 5 years and there is no evidence of recurrence.
CT scan showing good bony infill.

OPT showing good bony infill.
DISCUSSION
To explain the aggressive nature and its recurrence rate, the biochemical features of KCOT have been examined. There are certain growth factors that are seen particularly in KCOT which makes it more aggressive than other odontogenic cysts. A high level of EGFR expression is seen in KCOTs and this supports the view that they have an intrinsic growth potential that is not present in odontogenic cysts [5]. Increased levels of transforming growth factor alpha and epidermal growth factor are also seen in KCOT [5]. Intra-luminal hyperosmolality, collagenolytic activity in the cyst wall, synthesis of interleukin IL-6α and IL-1α by keratinocytes [5] along with tumour necrosis factor, causing raised level of prostaglandin and increased expression of parathyroid hormone-related peptide are thought to influence expansion of KCOT within bone and thus facilitate its unremitting growth [1].
The high recurrence rate of KCOT is believed to be due to a thin epithelial lining which tends to be fragile and difficult to enucleate in one piece. Forssell [6] felt that the most significant factor determining recurrence was whether the cyst was enucleated in one or several pieces. Other treatments such as decompression and irrigation, enucleation with Carnoy's solution and peripheral ostectomy have been used as well.
Decompression and regular irrigation of the cyst cavity produces inflammatory changes within the cyst lining and leads to modulation of epithelial type [6]. The inflammatory changes produced are probably secondary to oral communication [6]. The inflammation induces metaplastic change in the epithelium with the loss of parakeratinization [6]. Decompression and regular irrigation lead to conversion of the thin friable epithelium to a thickened lining with little adherence to the surrounding bone [6].
Histological examination in our case prior to decompression showed a thin band-like parakeratotic cyst epithelium, with the palisaded pattern of cuboidal or columnar epithelium.
Post decompression and irrigation, the epithelium had changed to a thick parakeratinized type, typical of radicular cysts at the time of cystectomy.
The conventionally accepted treatment of a KCOT eroding through the mandible and invading the soft tissue would be a radical resection of the cystic lesion and surrounding mandible including an overlying margin of normal tissue [7]. The surgical approach to the lesion reported here would have necessitated a lip split mandibulotomy, resection of the lesion along with the surrounding normal soft tissue leading to huge morbidity.
This case report demonstrates that modulating the epithelium through decompression and irrigation facilitates conservative management even in aggressive KCOT which has invaded the soft tissue. The disadvantages of the chosen treatment regime did involve multiple general anaesthetics and prolonged treatment time for the patient.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}