





Abstract
A lump in the scrotum is a common presentation in most surgical clinics. However, myoepithelial tumours may not be up on the list of differentials. Although they may look benign, myoepithelial tumours are rare and have malignant potential. Treatment of these tumours involved total excision and adequate follow-up in cases of malignancy. These groups of tumours have not been reported in the scrotum in the past, but their occurrence in the vagina may not come as a surprise bearing in mind the embryonic origin of both organs.
INTRODUCTION
Myoepithelial tumours represent a homogeneous group of rare tumours that arise commonly in the salivary glands and to a lesser degree in the breast. These tumours are more common in females from their early 20s to their 50s [1–3, 5–7]. A significant proportion (90%) arises from the major and minor salivary glands and the remaining from the submucous and submandibular glands [4]. Some studies reported that these tumours have been seen in the breast, lungs, skin, skull, pancreas, bronchus, oral cavity, nasopharynx, larynx, maxillary sinus and vulva [2, 3, 8, 9]. They occur most frequently on the limbs (75%) followed by head, neck and trunk. The presentation is a painless palpable mass. The authors did not come across any report of scrotal occurrence in their literature search. In this report the authors wish to report a case of myoepithelial tumour in the scrotum.
CASE REPORT
A 61-year-old male, referred to the surgical outpatients with a 6-month history of a large swelling on the right hemi-scrotum with recent increase in size and tenderness. He denied any constitutional or urinary symptoms. He has a background history of hypertension, controlled on medications, and left inguinal hernia repair. He was an ex-smoker and consumed ∼12 units of alcohol/week. Examination of the scrotum showed a firm roughly oval swelling on the right hemiscrotum, measuring ∼.9 cm by 1.6 cm by 1.2 cm, non-mobile, as although it was not attached to any scrotal structures, it was attached to overlying skin. There were no associated skin changes (Fig. 1).

Scrotal lesion shown by the arrow above.
The patient underwent excision of the swelling from the right hemiscrotum under local anaesthesia. Resection was easily achieved. Histology of the sample showed circumscribed encapsulated partly spindled and partly mesenchymal cellular neoplasm arranged in sheets, trabeculae and whorled nests with a background of hyalinized stroma. The cells had uniform spindled to ovoid nuclei with a vesicular chromatin pattern and prominent central nucleoli with ill-defined cell borders and amorphophilic, eosinophilic and clear cell cytoplasms. The cells were also strongly positive for S100 protein and strong but patchy positive for Pan, cytokeratin AE1/3. The tumour also showed focal nuclear positivity for P63 and EMA but negative for smooth muscle actin, desmin and caldesmon (Figs 2 and 3).
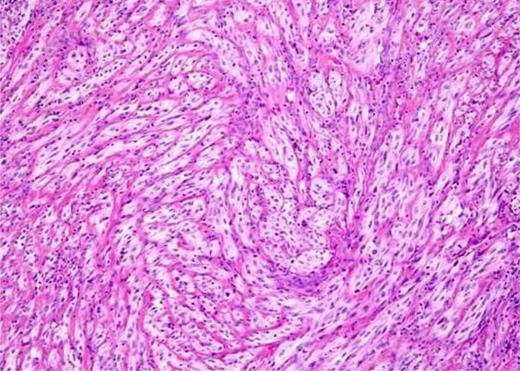
Myoepithelial cells stained and enhanced, negative for smooth muscle actin, desmin and caldesmon.
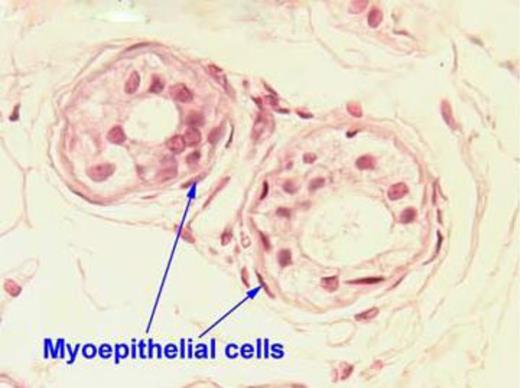
Cross section showing the myoepithelial cells.
A histological impression of myoepithelioma/mixed tumour was made. In view of the nuclear uniformity and low mitotic rate, the tumour was put on the benign end of the spectrum but with a potential of local recurrence. The patient was followed up for 2.5 years, he did very well postoperatively and had no recurrence or complaints.
DISCUSSION
Myoepitheliomas are rare tumours arising most frequently in the salivary glands but can also occur in soft tissues containing epithelial elements [3]. The vast majority of these tumours are benign but 10% may exhibit malignant potential [1]. The malignant variety is distributed equally in both males and females with a peak incidence from the third to fifth decade of life [3]. Normal myoepithelial cells are usually ovoid or spindle shaped with round nuclei and contains different quantity of cytoplasm. They are immunoreactive for S100 protein, smooth muscle actin, calponin and cytokeratins [1, 2, 5]. However, there are other S100/EMA-positive tumours [5].
It is worth noting that although majority of myoepithelial tumours are benign, 10% exhibit malignant potential with cellular structures exhibiting rough chromatin, increased cellular pleomorphism and increased mitotic rate [1, 7]. They also exhibit both epithelial and myoepithelial differentiation [7]. Some studies have also reported that other soft tissue malignant myoepithelioma has a high potential of becoming aggressive with a greater potential of metastasis [5, 10]. They can arise de novo or from pre-existing tumours. Pre-operative diagnosis is usually very difficult as differential diagnoses of the tumour include such diverse tumours as ossifying fibromyxoid tumour, malignant peripheral nerve sheath tumour, chondrosarcoma, epithelioid haemangioendothelioma and sebaceous cyst [2].
The clinical management of these rare tumours is unclear. Although, most mixed tumours/myoepitheliomas of soft tissue origin are both clinically and histologically benign, some recur locally. Michal and Miettinen [8] reported 1 case of metastasis and death from the tumour in a series of 12 patients with cutaneous and soft tissue myoepitheliomas. In a further published, one of the largest series by Hornick and Fletcher [9] reporting on over 101 patients, 33 patients on histologically proven benign disease, with a mean follow-up of 36 months, 6 [18%] developed local recurrences, with no distant metastasis. For benign tumours, resection and long-term follow-up is advised. However, no clear guidelines are mentioned as to what degree of resection margins are required to prevent local recurrences. The treatment for malignant myoepitheliomas/carcinomas involves complete resection of the tumour with free margins, remains the treatment of choice. However, there are no clear guidelines available regarding lymphatic basins, etc. [4, 8].
The role of local irradiation and chemotherapy though recommended is still unclear. This is perhaps due to paucity of studies. Only one case report and unpublished data mention the sensitivity of metastatic myoepithelial carcinomas to carboplatin and paclitaxel [10].
In their study, Hornick and Fletcher [9] described 31 patients with histologically proven myoepithelial carcinomas, reported a 42% recurrence rate with a rate of 32% for distant metastasis. Four patients died of metastatic disease, with deposits in the lung, mediastinum, spine, orbits, bone, brain and other unusual sites. In our case, the tumour exhibited low mitotic figures on histology, placing it on the benign end of the scale but we can be too certain as to the particular cell that gave rise to the tumour. In view of the histology report, we think it may have arisen from equal growth of both cell types. However, it is apparently important to note the possibility of recurrence of this tumour in the scrotum. The authors think that the occurrence of the tumour in the vulva as reported earlier may indicate increased possibility of the tumour recurrence in the scrotum in view of the close embryonic origin of both structures [2]. A high index of suspicion is relevant in the management of scrotal lesions.
CONFLICT OF INTEREST
None declared.

{kind=link}
{kind=link}
{kind=link}