





Abstract
Anterior belly of the digastric muscle (ABDM) variations have been reported to occur in as few as 2.7% to as many as 69.6% of individuals. Therefore, it is important to understand the anatomical diversity of ABDM variants, particularly with regard to head and neck surgery. The report documents a unilateral duplication of the ABDM with an oblique belly which crosses the midline. Measurements of muscle length, width, orientation and inferior surface area are documented. ABDM variants may cause confusion during surgeries, including submental lipectomy, rhytidectomy, surgical alteration of the cervicomental angle via partial resection of the ABDM, muscle transfer for reanimation of the mouth and submental artery flap procedures. Therefore, knowledge of this particular variant may aid in surgical planning as well as prevent confusion and disorientation during operations in the submental region.
INTRODUCTION
The anterior belly of the digastric muscle (ABDM) originates from the digastric fossa of the mandible and inserts at an intermediate tendon that serves as a shared attachment site with the posterior belly of the digastric muscle. When contracting together, these muscles function as synergists to depress of the mandible against resistance and elevate and stabilize the hyoid during deglutition and phonation. The ABDMs are typically considered to be symmetric bilaterally; however, diverse anatomical variations have been documented to occur, including duplications, triplications and quadrifications of the ABDM [1, 2]. ABDM bellies have been demonstrated to insert into the mylohyoid raphe or cross the midline and insert contralaterally [1, 2]. The ABDM has also been documented to present as a fractal, with one digastric giving rise to another smaller digastric from which other, even smaller digastric muscles originate [3]. In addition to the many types of ABDM variants, there is wide prevalence of ABDM variants, ranging from of 2.7 to 69.6% [4, 5].
CASE REPORT
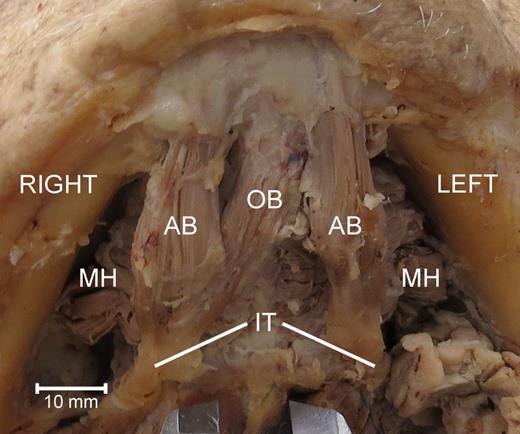
Inferior view of the variant digastric musculature demonstrating an oblique digastric belly variant crossing from the left digastric fossa of the mandible to the right intermediate tendon of the right digastric muscle. AB, anterior belly of the digastric muscle; OB, oblique belly of the anterior digastric muscle; MH, mylohyoid muscle; IT, intermediate tendon of the digastric muscle.
The ABDM on the left side was unremarkable. The length of the muscle belly, from the mandible to the intermediate tendon measured 33 mm. The breadth of the muscle, measured through the middle of the length of the muscle belly, was 10 mm. The visible area of the muscle belly was ∼280 mm2.
On the right side, there were two muscle bellies inserting at the intermediate tendon. The typical anterior muscle belly was, more or less, mirrored in its orientation to that of the right-sided muscle belly. Its length was 31 mm, width 13 mm, and visible area ∼340 mm2. An oblique muscle belly traveled between the right-sided intermediate tendon, sharing some muscle fibers with the right-sided anterior digastric belly, and the contralateral digastric fossa, sharing some muscle fibers with the left-sided muscle belly. The length of the oblique muscle belly was 41 mm, width 10 mm and visible area ∼220 mm2. At the intermediate tendon, the oblique belly formed an angle of 27° with the right-sided anterior belly. An angle of 38° was formed between the oblique muscle belly and the left ABDM at the mandible.
DISCUSSION
ABDM variations have been reported in as few as 2.7% to as many as 69.6% of individuals [4, 5]. Therefore, it is important to understand the anatomical diversity of ABDM variants, particularly with regard to head and neck surgery. The described variant has implications in procedures including submental lipectomy, rhytidectomy, surgical alteration of the cervicomental angle via partial resection of the ABDM, muscle transfer for reanimation of the mouth and submental artery flap procedures [2, 6–8]. Likewise, the ABDM is used as a surgical landmark for location of the lingual nerve and submandibular salivary duct [9]. It is also important to understand the diversity of ABDM variants in order to differentiate between anatomical and pathological structures common to the submental region including normal muscle tissue, submental lymph nodes, space occupying lesions and muscular asymmetries due to trigeminal nerve lesions.
CONFLICT OF INTEREST STATEMENT
None declared.
ACKNOWLEDGEMENTS
The authors thank: (i) Dr Richard Dey, Chair of the Department of Neurobiology and Anatomy at West Virginia University School of Medicine, (ii) the West Virginia Anatomical Board and (iii) the individuals who donated their bodies for the advancement of education and research. Without their support, this project could not have been completed. The research was supported by funding from two West Liberty University Faculty Development Grants and the WV Research Challenge Fund [HEPC.dsr.14.13].

{kind=link}