





Abstract
Cutaneous metastasis (CM) is an uncommon manifestation of visceral malignancies. Adenosquamous carcinoma of the gallbladder is a rare variation in gallbladder carcinoma (GBC), associated with worse prognosis. We present the case of a 56-year-old woman who presented with an inflamed lump on her abdominal wall. Computed tomography (CT) revealed a large mass from the gallbladder invading the abdominal wall. She underwent liver resection with regional lymphadenectomy. Pathology analysis revealed a 12-cm pT3N0 GBC. Hospital discharge occurred at post-operative Day 20. She recurred and died 10 months after surgery. Survival after the diagnosis of CM is dismal. The present case was a diagnostic trap. First, the patient's skin lesion presented as a cutaneous abscess and biopsy revealed a squamous cell cancer. A CT scan suggested a continuous mass involving the abdominal wall. CM was only suspected during surgery when no continuity between the tumour and the abdominal wall was identified.
INTRODUCTION
Cutaneous metastasis (CM) is an uncommon manifestation of visceral malignancies with a reported incidence of 0.7–9% [1, 2]. In extremely rare cases, it may be the first manifestation of the underlying disease. Breast cancer is the most common site for CM, followed by the lung, colorectal, renal, ovarian, and bladder cancers [3, 4].
Adenosquamous carcinoma of the gallbladder is a rare (<10%) variation in gallbladder carcinoma (GBC), being defined by the presence of a squamous component of 25–99% [5, 6]. The squamous variant of GBC is associated with an advanced T stage and worse prognosis [5, 6].
GBC commonly metastasizes to the liver and regional lymph nodes, whereas skin metastasis is extremely rare. In this study, we present the case of a GBC skin metastasis that was initially confounded with a non-melanoma skin tumour. Here, based on an extensive literature review, we discuss the frequency of GBC skin metastasis as well as the particularities of gallbladder adenosquamous carcinoma.
CASE REPORT

Inflamed lump on the right lateral abdominal wall initially considered as cutaneous abcess.
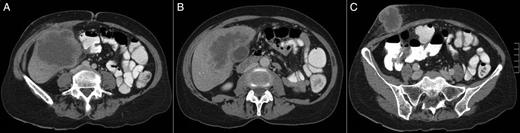
(A–C) A CT scan revealing a large hepatic mass invading the abdominal wall.

Intraoperative view after resection of segments 4B, 5 and 6 of the liver along with a regional hepatoduodenal ligament lymphadenectomy.

Final aspect of the abdominal wall.
Pathology analysis of the surgical specimen revealed a 12-cm adenosquamous gallbladder cancer invading the liver. There was no lymph node metastasis (0 out of 9). The skin lesion had no continuity with the liver mass and was thus considered a CM (pT3N0M1).
Recovery was uneventful and hospital discharge occurred at post-operative Day 20. Less than 1 month after hospital discharge, the patient noted a small enlarging and painful lump on her left shoulder. An excisional biopsy confirmed the lesion as another skin metastasis. Interestingly, as for the first cutaneous lesion, the squamous component was highly majority.
She received six cycles of weekly gemcitabine and a CT scan showed bilateral adrenal gland metastasis. Oral capecitabine was then started and 3 months later, the patient noted a 1-cm skin nodule at her left leg compatible with CM. A CT scan revealed an enlargement of the adrenal tumours, a 3-cm liver nodule and a 1.5-cm left upper lung nodule. Clinical status deteriorated progressively and the patient died 10 months after surgery.
DISCUSSION
Gallbladder carcinoma is a relatively rare and lethal gastrointestinal malignancy, with the majority of cases being adenocarcinoma. Primary carcinoma of the gallbladder includes the following histological types in a decreasing order of incidence: adenocarcinoma, adenosquamous carcinoma, squamous cell carcinoma and oat cell carcinoma [7]. Patients with adenosquamous cell carcinoma of the gallbladder most commonly present with a large mass replacing the gallbladder fossa. The bulky tumour is usually diagnosed at an advanced stage [8] with frequent invasion of the neighbouring organs, such as the liver, duodenum, stomach, colon, pancreas and extra hepatic bile ducts [9]. The liver is the most common site of invasion, and a higher proportion of liver infiltration is observed in patients with adenosquamous carcinoma when compared with those with adenocarcinoma [10]. GBC usually presents at an advanced stage, with metastasis in up to one-third of the patients, and a 5-year survival rate of <5% [2]. The overall prognosis of adenosquamous carcinoma/squamous cell carcinoma appears to be even worse with most patients dying within few months after the diagnosis [5].
While metastatic disease is common, extra abdominal spread, as in the present case, is extremely rare. Survival after the diagnosis of CM is dismal and usually <1 month [1], although it has been recently described the case of a patient alive and well after 25 months following her initial diagnosis, due probably to an aggressive strategy including chemotherapy, radiotherapy and surgery for multiple metastatic recurrences [1].
The present case was a diagnostic trap. First, the patient's skin lesion presented as a cutaneous abscess and was treated as such, and then the skin biopsy revealed a squamous cell cancer. Clinical examination and CT scan suggested a continuous mass involving the abdominal wall and liver. CM was only suspected during surgery when no continuity between the liver tumour and the abdominal wall was identified. It is interestingly to note that recurrence first occurred at skin and adrenals, which can be probably explained by the ectodermal origin of the medullary area.
In conclusion, there are limited examples of cutaneous metastatic GBC in the English literature. Also, there is limited information in the literature about adenosquamous carcinoma of the gallbladder. This case illustrates an unusual dissemination of GBC where the correct diagnosis has been made difficult by its unusual initial presentation, and the isolated presence of the squamous cell component at skin biopsy. Patient lived 10 months after resection which is superior to the mean survival reported in the literature in such cases. Although resection seems to improve survival as recently published, it cannot be recommended without previous multidisciplinary discussion. Patient's consent has been obtained.
The key learning points of this study are as follows:
CM is an uncommon manifestation of visceral malignancies.
Adenosquamous carcinoma of the gallbladder is a rare variation in gallbladder carcinoma associated with a worse prognosis.
CM can be a diagnostic trap and a high level of suspicion is necessary.
CONFLICT OF INTEREST STATEMENT
The authors do not have any financial and personal relationships with other people or organizations that could inappropriately influence this work.
REFERENCES
Author notes
This paper has been approved by all authors. Authors state that the manuscript has not been published before and is not under consideration for publication anywhere else.

{kind=link}
{kind=link}
{kind=link}