





Abstract
Orthotopic bladder reconstruction is becoming increasingly popular in patients who have undergone radical cystectomy. One of the rare complications is spontaneous rupture, which presents with various symptoms, but in particular, abdominal pain. We report a case of orthotopic bladder perforation in a patient who presented with the symptoms and signs of small bowel obstruction.
INTRODUCTION
Historically, ileal conduit formation following radical cystectomy has been the preferred type of urinary diversion. More recently, orthotopic bladder reconstruction has become increasingly popular, affording patients continence, maintaining as much normal voiding function as possible, with a more desirable body image and good quality of life [1–3].
One of the rare but serious complications of neobladder formation is spontaneous rupture. Such cases present in different manners with the overriding symptom being abdominal pain. We report a case of orthotopic neobladder perforation presenting with features of bowel obstruction.
CASE REPORT
A 71-year-old male had undergone a radical cystectomy and orthotopic neobladder formation 5 years previously, and was self-catheterising. He presented to the emergency department with a 24-h history of abdominal pain and distension. There was associated nausea and a reported decrease in urine production. Examination revealed a distended abdomen with some lower abdominal tenderness but no evidence of peritonism. Bowel sounds were absent. Relevant blood analysis revealed creatinine 354 µmol/l, WCC 15.9 × 109/l and CRP > 380. An abdominal X-ray revealed dilated small bowel loops, and a CT showed moderate volume ascites and distal small bowel obstruction with the transition being a thickened small bowel loop lying next to the neobladder (Fig. 1).
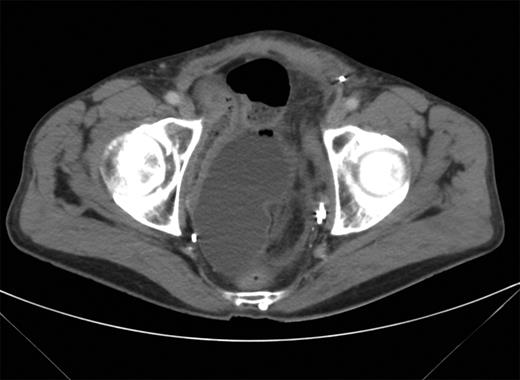
CT scan showing transition point of dilated bowel lying adjacent to the neobladder.
Conservative management was instituted (catheter, nasogastric tube) for presumed adhesional obstruction, and the patient was admitted under the care of the general surgical team. The urology team were contacted in light of the CT findings, and as the patient had not improved over a 24-h period, a decision was made to proceed with an exploratory laparotomy.
At surgery, there was a large amount of turbid urinary ascites, and the offending loop of small bowel seen on the CT was found to be stuck to a 5 mm perforation in the neobladder, at the junction of the afferent limb and the pouch. This was oversewn with an omental patch. The patient made a good recovery, creatinine normalized to 95 µmol/l, bowel function returned to normal and a cystogram at 10 days did not show any evidence of a leak.
DISCUSSION
Ileal neobladder perforation represents a rare but grave complication in such patients. A number of previous cases have been summarized by Ascaso et al. [4]. We describe a case of a previously unreported presentation of small bowel obstruction. Presenting features generally include fever and anuria, with abdominal pain being the main symptom. Possible causes of spontaneous rupture include overdistension, adhesions causing tearing of the neobladder wall and blunt trauma. In the vast majority of cases, exploratory laparotomy and repair is required; however, there have been two reported cases of successful conservative management [5, 6]. In this case, a segment of ileum became adherent to the neobladder, leading to bowel obstruction. It is difficult to postulate whether the adhesion caused tearing of the neobladder, or spontaneous rupture occurred first leading to subsequent adherence of the ileum.
This case highlights the importance of early urological input and a high index of suspicion of neobladder perforation in any such patient with abdominal symptoms, regardless of their nature.

{kind=link}