





Abstract
Post-EVAR type III endoleaks present a particular challenge as they carry a significant risk of rupture. We present a case of an 81-year-old gentleman, 10 years post-EVAR, with complex type III endoleak with component separation that was successfully treated with a combination of left renal artery chimney, aortouniiliac stent grafting and femorofemoral crossover bypass.
INTRODUCTION
Endovascular aortic aneurysm repair (EVAR) has revolutionized the treatment of abdominal aortic aneurysm (AAA) but the long-term durability is still uncertain. The EVAR 1 trial reported a re-intervention rate of 20% over 3 years in patients randomized to EVAR [1]. Type III endoleak can arise from fabric tear, graft disconnection or disintegration [2]. Secondary endovascular intervention is mandatory to prevent sac enlargement and rupture. We present a case of an 81-year-old gentleman, 10 years post-EVAR, who presented with a complex type III endoleak with component separation that was successfully treated with a combination of left renal artery chimney, aortouniiliac stent grafting and femorofemoral bypass.
CASE REPORT
An 81-year-old gentleman with a background of ischaemic heart disease, hypertension, hyperlipidaemia, polycystic kidney disease and previous right hemicolectomy for bleeding diverticular disease, underwent EVAR 10 years ago. He was on yearly follow-up with computed tomography (CT) scan and latest CT in 2012 showed a type III endoleak with aneurysmal sac of 10 cm in size. Both common iliac arteries were long and tortuous. He was electively admitted for a diagnostic calibrating aortogram in our CT hybrid angiography suite (Toshiba Infinix VC-i). Intra-operatively, digital subtraction angiography (Fig. 1) showed significant type IIIa endoleak with component separation on the left iliac limb. The old stent graft was <20 mm away from the left renal artery proximally (lowest visceral artery). He was discharged the next day and re-admitted 2 weeks later for a staged operation. Decision was made for a combination of left renal artery chimney, aortouniiliac stent grafting and femorofemoral crossover bypass.
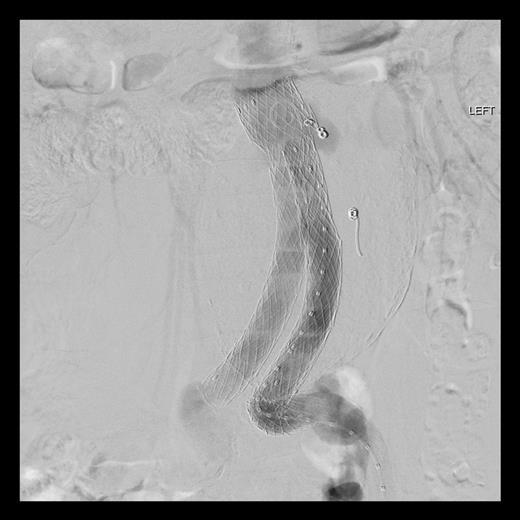
Digital subtraction angiography showing significant type 3a endoleak with component separationon the left iliac limb (black arrow). Both common iliac arteries were long and tortuous.
Surgery was performed in hybrid operating theatre. The aorta was accessed via bilateral groin cut-downs to expose both common femoral arteries. Intra-operatively, the type IIIa endoleak was excluded using a right-sided Cook aortouniiliac stent graft (AX1-1-36-116). The left renal arteries were cannulated from the left brachial artery. A PTFE-covered nitinol stent (Atrium V12) was advanced into the left renal artery and deployed in a chimney fashion. The left iliac limb of the stent was occluded using a 20 mm Amplatzer plug proximally and distally with Iliac Plug Zip 24 and 30 mm. Femorofemoral crossover bypass was then performed to complete the surgery. The completion angiography showed adequate sealing with no endoleak (Figs 2 and 3).
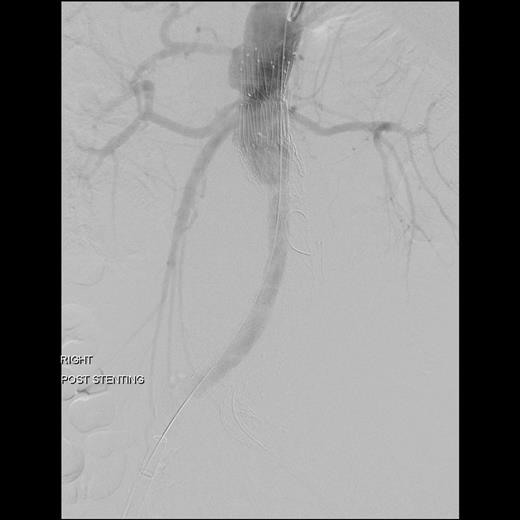
The completion angiography showed adequate sealing with no endoleak.

Angiography showing a femorofemoral crossover bypass.
DISCUSSION
Endovascular aortic repair for AAA has become popular and has shown satisfactory results since its introduction in 1986 [3]. EVAR is associated with reductions in early complications and mortality, as it avoids a large incision, full heparinization, extracorporeal circulation, aortic cross-clamping, interference with respiratory function and the need for massive blood transfusions [4]. However, there is still uncertainty about the long-term durability of EVAR. Endoleak remains one of the primary problems unique to EVAR.
Endoleak is defined as the persistence of blood flow outside the lumen of an endovascular graft but within an aneurysmal sac or the adjacent vascular segment being treated by the stent graft [2]. The reported incidence of endoleaks varies from 2.3 to 50% [5]. Type III endoleaks arise from a defect in the graft fabric, inadequate seal or separation of modular graft component [6]. It is clinically important as it communicates directly with the aortic lumen and will eventually lead to aneurysmal enlargement and high risk of rupture.
Appropriate procedural planning and device selection is critical to avoid endoleak. Umscheid et al. hypothesized that aneurysmal size, tortuosity of the vessels and late progression of aneurysmal remodeling and degeneration may contribute to graft distortion, modular separation and type III endoleak.
Type III endoleaks can be treated by open or endovascular surgery. Endovascular options include placing a new bifurcated endograft within the previous graft to seal the endoleak. In our patient, he has had previous abdominal surgery and multiple co-morbidites and thus the endovascular option was considered. Due to the long-tortuous left common iliac, a bifurcated, modular graft could not be placed. He also had a history of polycystic kidney disease with mild renal impairment. The option of the most straightforward procedure with minimal use of contrast to prevent contrast nephropathy was opted. The proximal landing zone was <20 mm from the left renal artery (lowest visceral artery). Thus the decision for a combination of left renal artery chimney, aortouniiliac stent grafting and femorofemoral bypass. The use of chimney stent graft allows preservation of blood flow to the left kidney, facilitating use of endovascular repair.
The use of a combination of left renal artery chimney, aortouniiliac stent grafting and femorofemoral bypass for type III endoleak has only been reported anecdotally. This treatment method extends the capabilities of endovascular salvage of difficult endoleak cases.
In conclusion, combination of aortouniiliac stent grafting and femorofemoral crossover bypass is a viable and safe option for treatment of type III endoleak. Chimney stent graft extends the capabilities of endovascular salvage for difficult type III endoleak cases.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}