





Abstract
Only 50% of abdominal aortic aneurysms present with the classic triad of hypotension, back pain and a pulsatile abdominal mass. This variability in symptoms can delay diagnosis and treatment. We present the case of a patient presenting with a unique combination of symptoms suggesting that decompression of urinary retention can lead to abdominal aortic aneurysm rupture.
INTRODUCTION
Ruptured abdominal aortic aneurysm (AAA) is one of the most dramatic emergencies and acute clinicians must be aware of it. However, frequently it presents with atypical symptoms leading to misdiagnosis and delay in treatment.
We present the case of a patient where a unique sequence of events culminated in a ruptured AAA.
CASE REPORT
An 84-year-old man presented with a 4-day history of worsening, cramp-like abdominal pain radiating into the back, later associated with abdominal distension and absolute constipation, in the absence of any urinary symptoms. He felt nauseated for 24 h but denied any vomiting.
Past medical history includes ischaemic heart disease, heart failure, asthma and gastro-oesophageal reflux. There was no past history of urinary problems.
Observations on admission where normal (blood pressure 130/85 mmHg, pulse rate 92 bpm, apyrexial 37°C, respiratory rate 15, saturations 98% on air, random blood glucose 7.5 mmol/l). The abdomen was distended with generalized tenderness but without guarding. There were no pulsatile masses. Auscultation revealed tinkling bowels sounds but no other abnormalities. Per rectal examination showed an empty collapsed rectum.
Blood tests including the haemoglobin (13.5 g/dl) where normal as was the erect chest X-ray. The abdominal X-ray showed minimal faecal loading but no other abnormality.
A computed tomography (CT) of the abdomen and pelvis was performed. This showed a grossly distended urinary bladder and compression of the sigmoid colon against the sacral promontory causing bowel obstruction (Figs 1 and 2, respectively) as well as a 4.9 cm abdominal aortic aneurysm without any signs of a rupture (Fig. 3). The plan was to consult our vascular colleagues regarding management of the AAA once the obstruction had settled.

The initial CT scan of the abdomen showing a large distended bladder.
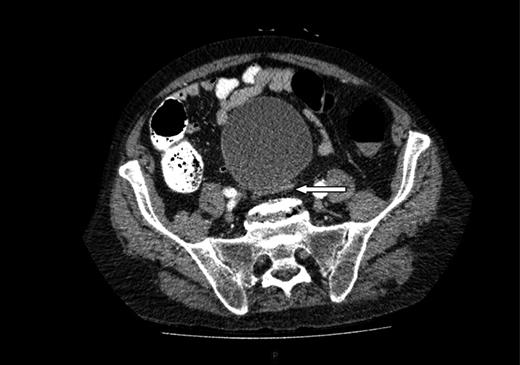
Further image of the same CT scan showing compression of the sigmoid colon against the sacral promontory (see arrow) behind the distended bladder.
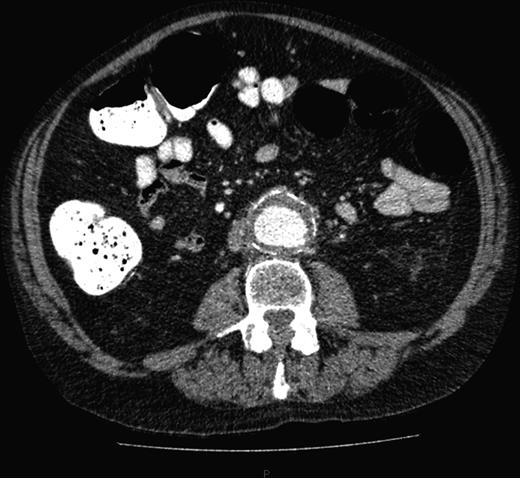
Abdominal aortic aneurysm with some wall standing thrombus but without any signs of rupture.
The patient was catheterized, immediately draining 2000 ml of clear urine relieving his obstructive symptoms and part of his pain. Unfortunately, this reprieve lasted only several hours and he once again complained about the same pain as before but increased in severity.
This time he was tachycardic and hypotensive with a much less distended but tender abdomen and still no palpable pulsatile masses. He was clinically stable enough to undergo a further CT scan of the abdomen and pelvis, now revealing a ruptured AAA (Fig. 4). We immediately transferred the patient to the regional hospital where he underwent emergency endovascular aneurysm repair on the same day.

Repeat CT scan of the abdomen, showing evidence of a contained rupture.
He remains well 3 months after his procedure.
DISCUSSION
The first to classify aneurysm and record their cause and treatment was the Greek surgeon Antyllus in the 2nd century AD. His original operation of proximal and distal ligation was the standard of treatment for over 16 centuries [1, 2].
Abdominal aortic aneurysms can be confusing. The classic combination of hypotension, back pain and a pulsatile abdominal mass is present only in 50% of cases. This pronounced variability of symptoms leads to misdiagnosis and treatment delay.
Aneurysm have been reported to present as renal colic, buttock pain, urethral obstruction, testicular pain, testicular swelling, peripheral neuropathy, paraplegia, hiccoughs, haematuria, inguinal mass, inguinal hernia, urinary retention and colonic obstruction [3–5].
When Rudolph Nissen performed an exploratory laparotomy on Albert Einstein for his recurrent episodes of upper abdominal pain with vomiting, he found a grapefruit-sized aneurysm. He wrapped the anterior portion of the aneurysm in polyethylene cellophane buying the patient 5 more years. When the aneurysm finally ruptured it presented as acute cholecystitis [6].
We present the case of a patient who presented with 4 days of abdominal pain radiating into the back, later on joined by distension, absolute constipation and nausea.
Following a CT scan of the abdomen and pelvis, he was found to have a distended bladder causing large bowel obstruction by pressing the bowel against the sacral promontory and what appeared to be an incidental 4.9 cm AAA without any signs of rupture (Figs 1–3).
Of course, the aneurysm ruptured following rapid decompression of the bladder.
Pryor reported that, of 44 patients admitted with ruptured AAA, 14 had back pains of up to 3 weeks duration prior to admission [7]. Our patient had abdominal and back pain for 4 days before presentation and the same pain but more severe after the rupture.
It is well reported that a ruptured AAA can cause urinary retention [5]. It is also known that rarely urinary retention can cause bowel obstruction and venous obstruction [8, 9].
To reconstruct the series of events, we believe that the back pain due to the imminent rupture of the aneurysm has caused acute (possibly on top of undiagnosed chronic) urinary retention. This then resulted in the large bowel obstruction. The clear chronological sequence of events suggests to us that the large distended bladder also prevented an imminent aneurysm rupture and that its fast decompression, draining ca. 2000 ml of urine, has facilitated the subsequent leak. Unfortunately, this is difficult to prove.
To the best of our knowledge, this is the first case reported of an abdominal aortic aneurysm presenting in this way.
In conclusion, the convoluted history of our patient should drive home the need to be ever vigilant when it comes to abdominal aortic aneurysms. They can present in any number of misleading ways and a persistently high index of suspicion is paramount.
Furthermore, it is good to keep in mind that a significant number of patients suffer with back pains as a prodromal symptom to imminent rupture. An urgent vascular consultation should be sought despite lacking radiological evidence of rupture in these patients.
Last but not the least, we feel that in patients presenting with urinary retention in the presence of a large AAA, a gradual, rather then rapid, decompression of the bladder combined with close monitoring is recommended.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}