





Abstract
The Foley catheter is described in the emergency treatment of penetrating cardiac injuries, and its intra-operative use to control bleeding while definitive measures for intravascular embolization are being made. We present the first reported case of the use of a urinary catheter to control haemorrhage in an extremity stab injury to obtain haemodynamic stability while awaiting definitive surgical treatment. This quick, easy and useful technique can be used for junctional vascular injuries and wounds with a narrow neck, and can be easily removed once in the operating theatre. This life-saving, simple and cost-effective technique ‘internalises’ the externally applied pressure to control massive haemorrhage while awaiting definitive operative intervention. The catheter can be sutured in place if the patient is to be transferred to another department or hospital.
INTRODUCTION
The Foley catheter is described in the emergency treatment of penetrating cardiac injuries [1], and its intra-operative use to control bleeding while definitive measures for intravascular embolization are being made [2]. It can be used to control bleeding from wounds in extremities and junctional zones, where bleeding vessels have retracted or simple pressure is ineffective at obtaining control due to the vessel depth and anatomy. Urinary catheters are immediately available in most Accident and Emergency Departments.
CASE REPORT
A fit and healthy 25-year-old right-hand dominant carpenter presented to the Accident and Emergency Department following a penetrating injury to his left wrist with a screwdriver. The patient was haemodynamically stable on admission, and on examination, the incision was ∼0.5 cm in width; however, there was obvious bleeding from the wound. The wound was a clean incised traumatic wound located on the volar aspect of the left wrist superficial to the tuberosity of the scaphoid. The bleeding was not controlled with pressure, and subsequently the patient became haemodynamically unstable with signs of shock. The patient was not able to be transferred to the operating theatre immediately due to another emergency case already in the theatre which resulted in a 20-minute delay, and the patient remained unstable despite fluid resuscitation. The decision was made to tamponade the bleeding with a sterile catheter, in an attempt to control the haemorrhage while awaiting definitive treatment. The method is as follows: insert the catheter tip into the wound under an aseptic technique and inflate the balloon as appropriate to the wound size. The wound can be lined with gauze swabs to aid friction. If necessary it can be slightly over-inflated. Spigot or clamp the catheter and re-apply direct pressure to the wound and balloon with sterile dressings. The pressure is transmitted within the wound providing temporary haemostatic control en route to the operating theatre (Fig. 1).
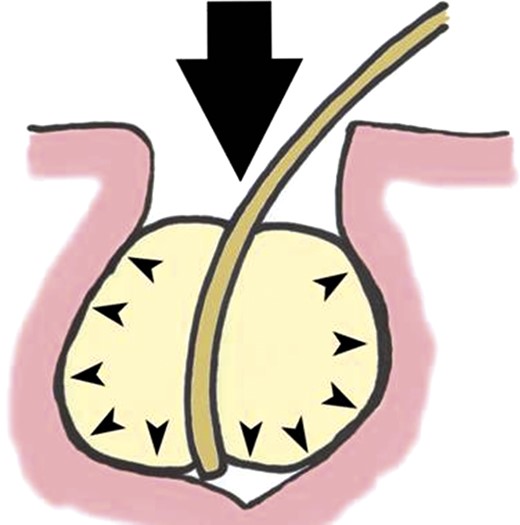
Schematic diagram showing transference of external pressure by balloon (A) to the internal aspect of a wound (B).
In this particular case, we managed to attain haemorrhage control and haemodynamic stability in the precious 20-minute period while awaiting wound exploration and definitive treatment in the operating theatre.
The intra-operative findings were bleeding from the venae comitantes of the distal radial artery, which were subsequently ligated.
DISCUSSION
The urinary catheters are accessible and familiar to junior doctors in the Accident and Emergency Department (Fig. 2). This quick, easy and useful technique can be used for junctional vascular injuries and wounds with a narrow neck, and can be easily removed once in the operating theatre. This simple and cost-effective technique ‘internalises’ the externally applied pressure to control massive haemorrhage while awaiting definitive operative intervention. The catheter can be sutured in place if the patient is to be transferred to another department or hospital [3].
Urinary catheter with inflated balloon.
This technique is useful when first aid measures such as elevation, direct pressure, haemostatic agents and fluid resuscitation fail to achieve haemodynamic stability in the bleeding patient while awaiting definitive surgical treatment.

{kind=link}
{kind=link}
{kind=link}