





Abstract
Signet cell carcinomas of the colon are well documented in the adult population, but this cancer incidence is very low in the adolescent population. A 17 year old male child presented with one month of progressive abdominal pain. CT scan of the abdomen showed significant abnormality involving the ascending colon characterized as marked mural thickening. Biopsy results indicated signet ring cell carcinoma. Signet cell carcinoma is presumed to be caused by genetic mutations just like the other colorectal cancers. Treatment for signet cell carcinoma is the same as other colorectal cancer. Surgery is part of the standard management of patients with colon and rectal cancer stages I, II and III. Signet cell cancer has a poor survival with the median survival period of about 9 months. The incidence among adolescence is much lower than that of the adult population.
INTRODUCTION
Signet cell carcinoma of the colon and rectum are rare aggressive tumors that are known for their spread to other organs and the peritoneum. While well documented in the adult population, this topic is not well published in the adolescent population. They account for 0.8% of the surgical patients with colorectal cancer (1). The disease is seen more in males with a male to female ration of 1.1:1 (2). The incidence is higher in the adult population and is usually diagnosed at a younger age when compared to other colorectal cancers. The infrequency of the disease among the adolescents makes the diagnosis more difficult and the prognosis less favorable. We report a case of signet cell colon cancer a in a 17 year old child.
CASE REPORT
A 17 year old male child presented with one month of progressive right sided abdominal pain and swelling. He reported that eating and playing sports aggravated his pain. His social and family history was significant only for occasional smoking. Vital signs were all within normal limits on admission. Physical examination revealed a pleasant child without any distress. Abdominal examination revealed a soft non tender abdomen with normal bowel sounds. A firm mass was palpated in the right upper quadrant. Laboratory examination revealed a white blood cell count of 11.5 per cubic millimeter, hematocrit of 35%, and platelet count of 395,000 cells/cubic millimeters. Mean corpuscular volume was significant with 56 fl. Electrolytes were normal except for sodium of 132 meq/liter. Liver function tests, pancreatic enzymes and urine analysis were normal. The ultrasound of the abdomen revealed a non peristalsing bowel loop which had a configuration strongly suggestive of intussusceptions of the right side of the abdomen. This ultrasound was followed by a CT scan of the abdomen, which showed significant abnormality involving the ascending colon characterized as marked mural thickening having a low density relative to muscle. Colonoscopy was done which showed edematous, necrotic mucosa of the colon with ulceration. Biopsy results indicated signet ring cell carcinoma. Complete investigations confirmed T4 N2 M1 signet ring cell carcinoma. The patient underwent right colon resection with ileocolic anastomosis followed by with 20 cycles of FOLFOX-6.One year later, patient presented with symptoms and signs of bowel obstruction. Follow up CT-Scan was done which indicated cancer recurrence in distal pelvis warranting further investigations. Fine needle aspiration was positive for malignant cells consistent with recurrence of signet ring cell carcinoma. Therefore the patient then underwent a diagnostic laparoscopy and debulking. Unfortunately the patient passed away one week after debulking procedure.
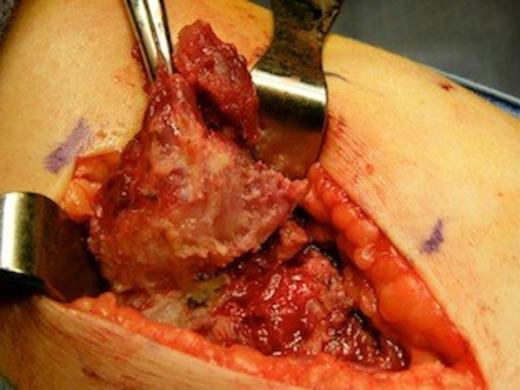
Signet ring cell carcinoma
DISCUSSION
Signet cell cancer of the colon is a rare subtype of colon cancer, where abundant intracytoplasmic mucin pushes the nucleus to the periphery giving a signet ring appearance. In order to meet the definition, signet cells should account for at least 50% of the cells. There are reports that signet ring cell carcinoma has been increasing in incidence (2) and currently Signet cell carcinoma accounts for 0.7% of the colorectal cancer. Patients are often noted to be younger compared to the non-signet cell tumors of the colon. Median age is about 59 years when compared to the non signet cell cancer, where the median age is about 61 years (2). Our case is very significant because of very young age of presentation of this cancer.
Signet cell carcinoma is presumed to be caused by genetic mutations just like the other colorectal cancers. Micro satellite instability (MSI) is a well-recognized phenomenon in colorectal cancer. Micro satellite unstable tumors can be divided into two distinct MSI phenotypes: MSI-high (MSI-H) and MSI-low (MSI-L). Signet cell carcinoma has a high level of MSI (MSI-H) (3). Incidence of K-ras mutation is lower compared other colorectal cancer (4).
The most common presenting symptom is abdominal pain. Other symptoms include rectal bleeding, change on bowel habits and weight loss. About half of the of signet cell ring cell carcinomas were found in the rectum and colon, most predominant site being the right hemi colon in about 29%. Left colon comprises about 15% and approximately 9% of the tumors are noted in the transverse colon (5). A majority of the signet cell carcinomas initially present with the distant metastasis in about half of the patients. Presentation in children does not differ significantly from the adults (6).
Surgery is part of the standard management of patients with colon and rectal cancer stages I, II and III. Some selected patient may undergo surgery in stage IV. Chemotherapy is the standard adjuvant therapy for stage III colon cancer, and chemo radiotherapy is the standard adjuvant therapy for stage II and III rectal cancer. However, for stage IV colon and rectal cancer, chemotherapy alone may be appropriate and in bulky tumors surgery/radiation can be used for palliation. The median survival period is about 9 months. Comparing the respective signet ring cell carcinoma to the high-grade non-signet cell rectal carcinoma the five year survival rates are nearly equal. One of the reasons for poor survival period is that most of the signet cell colon cancers are diagnosed at more advanced stages (7).
In conclusion, Signet cell carcinoma of the colon, has a poor prognosis. It can affect patients of any age. The incidence among adolescence is much lower than that of the adult population. Early curative resection has significantly improved survival rates compared to the late curative resection groups and to the other groups.

{kind=link}