





Abstract
Carcinoid tumours are rare with an incidence of 5.25/100,000. They predominantly originate in the gastrointestinal tract (50-60%) or bronchopulmonary system (25-30%). Common sites of metastasis are lymph nodes, liver, lungs and bone. Spinal metastasis are rare, but has been reported in patients with symptoms of spinal cord compression including neurological deficits. We report a rare case of carcinoid metastasis with spinal cord compression, in a 63-year-old man, presenting with a one-year history of back pain without any neurological symptoms. The patient underwent a two-level decompressive laminectomy of T10 and T11 as well as piecemeal tumour resection. Post-operatively the patient made a good recovery without complications.
INTRODUCTION
Carcinoid tumours represent a spectrum of slow-growing malignancies that arise from neuroendocrine cells characterised by their ability to produce and secrete peptides. The incidence increases with age, and most patients are diagnosed in the fifth decade of life (1,2).
The spinal canal is an uncommon site of metastasis resulting in spinal cord compression and potentially neurovascular compromise. To the best of our knowledge spinal metastasis of a carcinoid tumour is unreported in the absence of neurological symptoms. Here, we present a case report on such an atypical occurrence.
CASE REPORT
A 63-year-old man presenting with right upper quadrant pain was, following a CT of the chest, abdomen and pelvis, found to have a lesion in the lung and multiple liver metastases.
A liver biopsy was performed. Histological examination showed a low-grade neuroendocrine “carcinoid” tumour, most probably of lung origin.
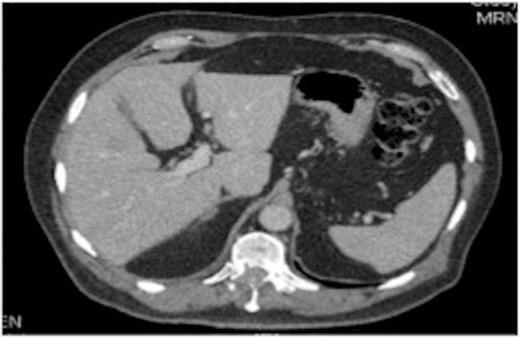
Original thoracic CT scan, which was performed 2 months prior to the MRI, shows the spinal metastasis
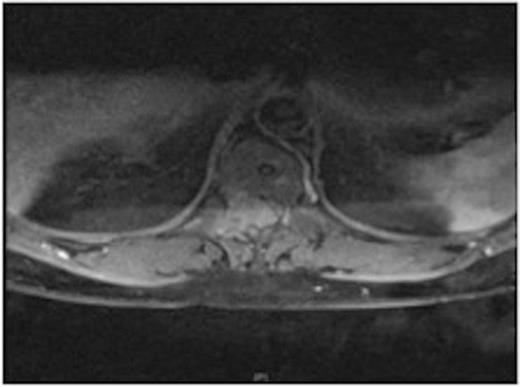
MRI showing the extra-dural tumour and extension into the soft tissue of the back
A one-year history of lower back pain, which was initially thought to be due to his liver metastasis, was investigated further with a full spine MRI scan. The scan revealed a large T10-11 extra-dural tumour with erosion of the T12 pedicle and extension into the soft tissue of the back. As a result of this discovery, the patient was referred for radiotherapy. Prior to commencement of this the oncologist requested a neurosurgical opinion from us.
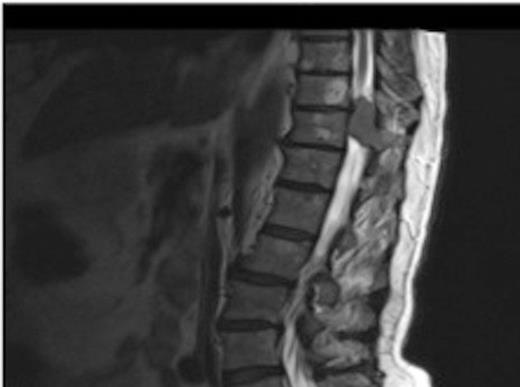
MRI showing the T10-11 extra-dural tumour with erosion of the T12 pedicle
On review of the original thoracic CT scan, which was performed 2 months prior to the MRI, the tumour was distinguishable but, as the spine is such a rare location for carcinoid metastasis, it was initially unreported.
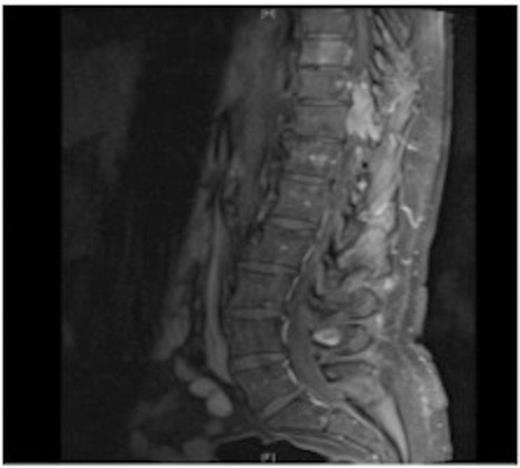
MRI showing the T10-11 extra-dural tumour with erosion of the T12 pedicle
Due to the low-grade nature of the tumour and the spinal cord compression the advantages and disadvantages of surgery versus radiotherapy were discussed with the patient who then agreed to have the tumour surgically removed.

MRI showing the T10-11 extra-dural tumour with erosion of the T12 pedicle
The patient underwent a two-level decompressive thoracic laminectomy and complete macroscopical excision. An intra-operative smear exhibited carcinoid tumour characteristics.
Post operatively the patient made a good recovery and today, more than 2 years post-surgery, the patient is still doing well without any neurological complaints.
DISCUSSION
In this case the large discrepancy between the size of the tumour and the complete lack of neurological deficits is noteworthy. Even though low back pain is a very common complaint, we feel, it should be taken more seriously in patients with an oncological diagnosis. Urgent radiological imaging should be considered in the form of a full spine MRI. In this instance a further delay in investigation would have jeopardised the good functional outcome.
It is also noteworthy that due to the rare occurrence of spinal metastasis from carcinoid tumours, especially without any neurological symptoms, the visible spinal metastasis on CT was, in this case, initially overlooked.
The absence of neurological symptoms, in this case, must be attributed to the slow growing nature of the tumour. A charachteristic, which is common for carcinoid tumours and which makes surgical de-bulking to prevent morbidity a rational part of the treatment plan (3).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}