





Abstract
Maxillary sinus foreign bodies are commonly due to penetrating trauma and iatrogenic events. A foreign body is usually identified during initial assessment and subsequently removed. We present a rare method of maxillary sinus trauma with retained and subsequent discharged foreign body twelve years following the initial injury.
INTRODUCTION
We discuss an unusual presentation of maxillary sinus trauma with retained and subsequent discharged foreign body (FB) after twelve years.
CASE REPORT
A normally fit and well 31 year old female was referred by her general practitioner to the ENT department with sinusitis unresponsive to treatment in the community and an unusual history.
In December 1999 the patient attended a public house where she greeted a friend playing snooker. Her friend picked her up in his left arm; in his right hand, he held a snooker cue. When dropping her back down onto the floor the snooker cue entered her mouth and she suffered a penetrating injury to the right side of the gingivo-labial sulcus to an unknown depth. The snooker cue was promptly removed at the scene and the patient attended A&E where she was assessed and discharged home with analgesia. There was extensive bruising to her right cheek for 4 weeks after the trauma.
She had suffered with right sided rhinorrhea and episodes of sinusitis since the injury, which were treated by antibiotics in the community. She also complained of right-sided facial pain and underwent dental surgery for tooth extraction with no relief of symptoms.
She attended her GP in August 2011 after a coughing episode resulted in a small green cylindrical object entering her oral cavity. The object was consistent in appearance with a snooker cue tip. She then developed a severe case of sinusitis.

Foreign body- snooker cue tip
The patient then attended our clinic. Clinical examination and subsequent naso-endoscopy showed evidence of a right sided nasal obstruction with polypoidal mass within the nasal cavity. The patient underwent CT scan sinuses, which showed a well demarcated air defect in the extensively thickened sinus mucosa with large polypoidal mass. Evidence of entry of the cue was seen as a defect in the anterolateral wall of the right maxillary sinus and absent upper medial wall. No FB was seen.
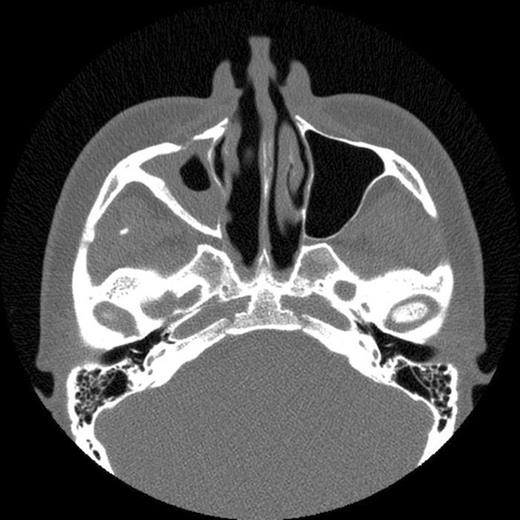
CT scan showing fracture of the anterolateral wall of the right maxillary sinus and absent upper medial wall

CT scan showing extensive polyp mass in right maxillary sinus with extension into right nasal cavity
The history and CT scan results suggest that following penetration of the snooker cue into the gingivo-labial sulcus it had broken through the right anterolateral maxillary wall and upper medial wall. On withdrawal of the snooker cue, the cue tip had broken off in the maxillary sinus. The FB had then caused localised inflammation resulting in episodes of sinusitis and facial pain. The FB had subsequently been discharged during a coughing episode 12 years later.
The patient was started on a steroid nasal spray and underwent endoscopic right sided sinus surgery with removal of polypoidal mass from the right nasal cavity and maxillary antrum. Histological analyses were consistent with chronic hypertrophic rhinitis with polyp formation.
DISCUSSION
After a search of the literature, we were unable to identify a similar case of maxillary sinus trauma with retained FB.
Reported cases of snooker cue injuries are rare. A case of self-inflicted penetrating orbital injury due to a snooker cue through the oral cavity resulted in the cue passing the maxillary sinus and the orbital floor causing traumatic optic neuropathy with partial visual loss (1).
Another case of snooker cue trauma involved an orbitocranial injury penetrating through the eye leading to intracranial haemorrhage (2). A report of severe temperofacial infection was secondary to an occult foreign body following snooker cue injury (3).
Maxillary sinus foreign bodies following trauma are commonly secondary to gunshots and projectiles, Harvinder et al (4) described a case of an arrow in the maxillary sinus following a fishing accident, which was successfully removed surgically.
The unusual presentation of a retained and eventual discharged FB highlights the need for thorough initial history and examination in facial trauma to guarantee that a FB is not present. When available, assessment of the penetrating object post-trauma to ensure there are no missing parts is invaluable.
It underlines the need for a detailed history in patients presenting with recurrent sinusitis. Although the history is very unusual, the knowledge that the patient had previous trauma and then subsequent infection close to the trauma site may have eluded that a FB was present.
It also draws attention to the management of patients with chronic sinusitis and current guidelines. Guidelines for primary care physicians are available from the evidence–based NHS PRODIGY site (5). They advise referral to secondary care when there is recurrent or chronic sinusitis, progressive or unremitting facial pain, and nasal polyps which are causing significant nasal obstruction and patients have had a trial of intranasal corticosteroids for 3 months which was ineffective. Given the recurrent sinusitis and facial pain this patient meets the criteria for referral to secondary care.
In summary, this unusual case of nasosinus trauma highlights the need for thorough history and examination when suspecting FB in penetrating injuries and allows reflection on current guidelines for sinusitis.

{kind=link}
{kind=link}
{kind=link}