





Abstract
Various anomalies of the inferior venacava (IVC) have been reported in the past. Amongst, the absence of IVC is one of the less frequently reported anomalies. The absence can be complete or partial, confined to the hepatic, supra-renal or infra-renal segment of IVC. It is still a controversy, whether these conditions are true embryonic anomalies or the result of perinatal IVC thrombosis.
A man in his mid 30’s presented with absence of the infra-renal IVC and both common iliac veins. The right renal vein is replaced by a long tortuous vessel, similar to the appearance of collateral vessel. He presented with extensive varicose veins on the anterior abdominal wall, severe varices of right leg with ulcer. A coronal multiplanar reconstruction CT imaging was used to document the anomaly.
Prior knowledge of this anomaly is vital, especially if these individuals are subjected to undergo cardiac procedures via femoral vein access.
INTRODUCTION
The recent development in cross sectional imaging and advanced radiological techniques is an asset in recognising the anomalies of IVC & its tributaries as an incidental finding in asymptomatic patients.
The clinical presentation of the patients varies from lower extremity varicose veins, stasis and dermatitis including idiopathic, recurrent deep venous thrombosis since adolescence. The other major clinical complication of this condition may present as retroperitoneal hemorrhage as a result of ruptured collateral vessels or mass effect of the paraspinal collateral circulation.
The absence of the infra-renal IVC and the right renal vein is the most severe and infrequent abnormality in anomalies of IVC. Awareness of this condition is vital, especially if these individuals are subjected to undergo cardiac procedures via femoral vein access. Moreover, an accidental ligation of the right renal collateral may deprive the functions of right kidney.
CASE REPORT
A man in his mid 30’s was referred with complaints of right lower limb pain, swelling, varicose veins with a venous ulcer. He had a past history of perinatal transfusion for Erythroblastosis foetalis during his childhood. He has been suffering from right lower limb varices since his childhood and was treated for recurrent episodes of deep venous thrombosis.
Physical examination revealed multiple large varicose dilatations in right lower limb, collaterals seen in the right anterior and lateral wall of the abdomen.
Contrast enhanced abdominal computed tomography rendered the hypoplastic renal segment of IVC along with the absence of infra-renal IVC.
The absence of the right common iliac vein, right external & internal iliac veins and right proximal common femoral vein was also seen. Left external & internal iliac veins drains into the retroperitoneal collaterals due to absence of left common iliac vein. The hepatic veins demonstrate drainage into intrahepatic segment of IVC (Fig. 1).
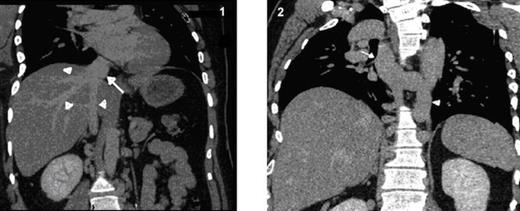
Coronal MPR CT image shows hepatic veins (arrow heads) seen draining into the intra-hepatic segment of IVC (arrow)
Dilated and tortuous azygous & hemiazygous veins (Fig. 2), with multiple prevertebral and paravertebral collaterals (Fig. 3) as well as superificial collateral veins in the abdominal wall (Fig. 4) were seen. Left renal vein is draining into the hypoplastic segment of IVC (Fig. 5).
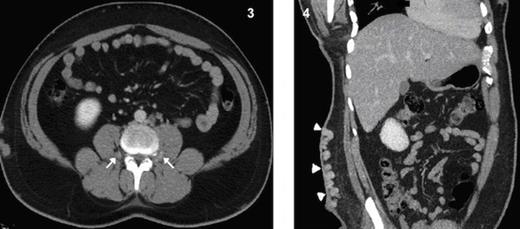
Coronal MPR CT image shows grossly dilated azygous vein (arrow) and hemiazygous vein (arrow heads)
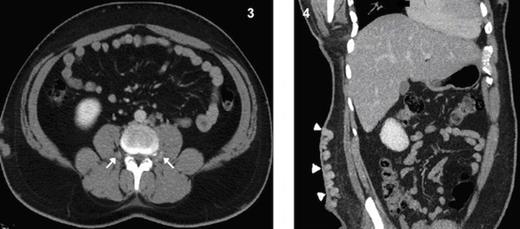
Axial CT image shows collateralization of paraspinal veins (arrows) Fig 4. Coronal MPR CT image shows massive varices of superficial collateral veins at the abdominal wall.

Coronal MPR CT image shows a long left renal vein seen draining into the intra-hepatic segment of IVC. Fig. 6 Coronal MPR CT image shows a right renal collateral vessel draining into hypoplastic segment of IVC.
The right renal vein is absent represented by long tortuous collateral draining into hypoplastic segment of IVC (Fig. 6) and multiple collaterals draining into the retroperitoneal venous plexus (Fig. 7). The right great saphenous vein exhibits drainage into the distal part of right common femoral vein (Fig. 8).
The renal function tests including blood urea, nitrogen and creatinine levels were in normal limits.
DISCUSSION
A concise review of the embryogenesis is recommended to better understand the possible causes of the anomalies of IVC. Phillips (1) has summarised the work of early investigators in a comprehensive manner. The normal inferior vena cava is composed of four segments: hepatic, supra-renal, renal, and infra-renal. The proximal right vitelline vein gives rise to the hepatic sinusoids that derives the hepatic segment. The post-hepatic IVC develops between the sixth and eighth weeks of embryonic life as a composite structure formed from the continuous appearance and regression of three paired embryonic veins, the posterior cardinal, the subcardinal, and the supracardinal veins. The supra-renal segment develops from the right subcardinal vein and the infra-renal segment develops from the right supracardinal vein. The renal segment is derived from the anastomosis between subcardinal and supracardinal veins. IVC anomalies result from abnormal regression or abnormal persistence of embryonic veins. Persistence of the right postcardinal vein with regression of the supracardinal vein results in the well-known anomaly Retrocaval ureter (1).
The absence of infra-renal IVC is a rare anomaly (2). In this anomaly, the developmental insult involves the supracardinal system (2). In this patient, neither the right postcardinal vein nor the supracardinal vein persisted. D’Archambeau (3) and Milner (4) have proposed that the absence of the infra-renal IVC results from intrauterine or perinatal thrombosis of the IVC and is not of embryonic origin. This suggestion is supported by the work of McDonald et al. (5), who reported a series of 10 patients with renal vein thrombosis. Seven were found during the perinatal period. Swaiman et al (6) suggested that due to the fact that supracardinal veins form last, the supra-renal and renal IVC may form normally from the subcardinal veins, and the infrarenal segment may not develop because of a later insult to the supracardinal veins. But, as Bass et al (2) pointed out, it is true that this construction does not explain the failure of the postcardinal veins to persist, as occurs in retrocaval ureter.
However, anomaly of the IVC has been identified as one of the important causes of deep vein thrombosis (DVT) in the lower extremities, involving iliac veins, in young patients. This is strongly evidenced by Obernosterer et al (7) and supported by Gayer et al (8). The original work of Obernosterer reported 31 of 97 patients with DVT, demonstrated thrombotic occlusion of iliac veins. Five of 31 patients had an anomaly of the inferior vena cava. Anomalies were missing inferior vena cava, hypoplastic hepatic segment, and missing renal or infra-renal segments with all the five patients being significantly young.
In this patient, in addition to the absence of the infra-renal IVC, an anomalous right renal vein is present. It is represented as a long tortuous vessel that looks more likely as a collateral vessel rather than the actual renal vein. Variations of renal veins are rare compared to the renal arteries. Variations of right renal veins are more common than left renal veins (9). Janschek et al (10) reported renal vein variations being more common on the right side (23%) than on the left (6.7%). Several variations in right renal veins are reported including multiple renal veins and doubling. But none reported a combined absence of infra-renal segment of inferior vena cava with anomalous right renal vein.

{kind=link}
{kind=link}
{kind=link}
{kind=link}