





Abstract
Teratomas are the benign tumours, which may occur anywhere in the body. Development of these lesions in the oral cavity is extremely rare. In the oral cavity, they usually arise in the midline, in the floor of mouth. Infrequently, they may be seen in the tongue proper. We hereby, present a case of swelling tongue in 56 years female diagnosed as teratoma.
INTRODUCTION
Teratomas are benign neoplasms composed of all the three germinal layers. Around 80% are located in the ovaries and sacral lesions, 7% are seen in head and neck region, only approximate 1.6% of these tumours are found in oral region. Pure oral presentation in the tongue is extremely rare. Only a few number of cases have been reported in the literature so far (1).
CASE REPORT
A 56 years old female presented with swelling on the dorsal surface of tongue. Examination revealed a firm, rubbery, non-tender 3x2x2cm sessile swelling with no induration or ulceration (fig 1).
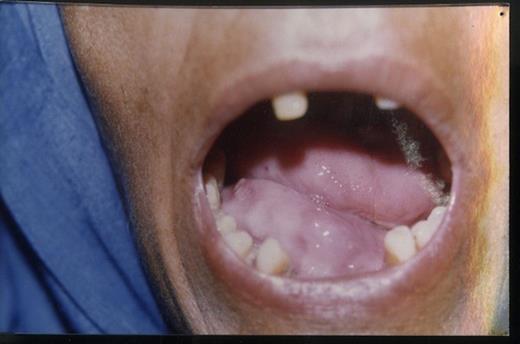
Swelling on surface of tongue
She noticed this swelling 6 months previously, which more recently increased in size. Lately, she experienced difficulty in moving tongue, resulting in globbus sensation and dysphagia. General examination of the patient revealed average built, pulse rate 80 beats/min with regular rhythm, BP 130/90 mm Hg, RR 24 breaths/min. There was no history of fever, night sweats and weight loss. Jaundice, cyanosis and oedema were absent. Computed tomography revealed a 3x2 cm cystic anterior lingual structure, the wall of which was thin and regular with a content consisting of homogenous fluid. There was no bone involvement. With a clinical diagnosis of dermoid cyst an excision biopsy was performed. Histopathological findings consisted of cyst wall lining of stratified squamous epithelium with sebaceous glands, blood vessels, muscle and cartilage in the underlying connective tissue, and a diagnosis of teratoma was made (fig 2). No evidence of malignant transformation was noted. One year after surgical removal of the lesion, there was no sign of recurrence.
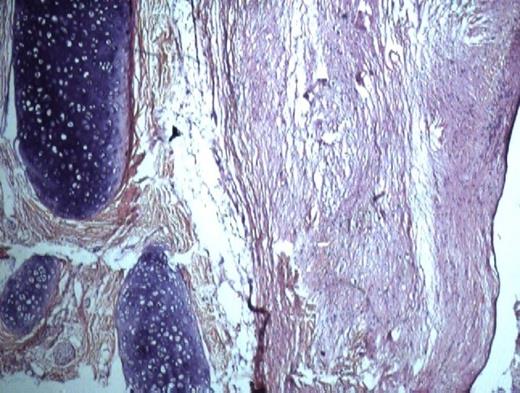
Histological specimen
DISCUSSION
The tongue is derived from two separate embryologic origins. The anterior two thirds is derived from ectoderm and posterior one third is from endoderm. The anterior two third s originate from paired lateral lingual swellings, which are contributed by first branchial arch. These swellings fuse in the midline to form the tuberculum impar. The posterior one third of the tongue arises from the hypobranchial eminence, which is made up of mesoderm of the second, third and a portion of the fourth pharyngeal arches. Congenital dermoid cysts arise from epithelial rests trapped during midline fusion of these branchial arches whereas acquired dermoid cyst arise from epithelium implanted during trauma and they occur at the sites away from midline. The terms teratoma, teratoid cyst and dermoid cyst have been used interchangeably to describe a wide variety of lesions by some authors. Meyer has classified these cyst as epidermoid, dermoid and teratoid. Epidermoid cysts are lined with simple squamous epithelium and surrounding connective tissue. Dermoid type cysts contain skin appendages whereas teratoids contain epithelium lined mesodermal or endodermal elements such as bone, teeth, muscle, mucous membrane (2).
Teratomas of the oral cavity are divided anatomically depending on their location. They can be sublingual, geniohyoid and lateral (3). The other differentials which are encountered at these sites are ranula, lymphangioma, angioma and lipoma (1). Teratoma is a tumour, which contains disorderly arranged tissues and organs. There is an epithelial lined cavity containing mesodermal as well as endodermal derivatives like muscle, intestinal mucosa, respiratory mucosa, fibres, bone and blood vessels etc. Teratoma of tongue may exhibit skin, hair, bone, cartilage or mucous membrane on the surface (7). The rarity of teratoma has been stemmed from the fact that it is not located along embryonic fusion line and it does not involve the floor of the mouth (4). Teratoma in the head and neck region are rare, comprising 1-10% of cases. Very few numbers of cases have been reported so far. They probably arise from totiopotent embryonic tissue that has been displaced during ontogeny (8).
A good patho-radiological correlation is required to confirm the diagnosis. Ultrasonography establishes the presence of solid and cystic components and can differentiate cyst from surrounding tissue. By far MRI has been proven to be superior among imaging modalities, as it can locate exact position, extention and demarcations of the lesion (1). Because of their avascular character, teratoma do not enhance with administration of contrast material and thus can cause diagnostic confusion with choriostoma, endodermal sinus tumours and granular cell tumours. Because oral teratomas are well defined, complete excision is usually possible. Recurrences are very rarely seen in head and neck teratomas. Most of the times, these tumours are benign but may result in high degree of mortality and morbidity due to variations in their size and location. If large enough, they may cause airway obstruction, respiratory distress, dysphagia, difficult in eating and pain due mostly to infection in the lesion. In malignant teratoma radio-chemotherapy is used after surgical removal of the tumour(5). Alphafetoprotein( AFP) has been shown to be reliable indicator of disease activity and some authors advocate investigating teratoma recurrence by doing serial serum AFP levels. They have been shown to increase in teratocarcinoma (6). Though teratoma has been reported in infants so far it is unusual with the site not being the midline. Malignant change was not seen. Patient responded better after complete surgical excision of the lesion. Though rare, teratoma should be considered in the differential diagnosis of tongue masses.

{kind=link}
{kind=link}