





Abstract
There have not been any cases published of idiopathic muscular hypertrophy of the gastrointestinal tract in the past 20 years, mainly because it is a very rare condition of unknown aetiology. It is usually asymptomatic and presents mostly in the oesophagus of adult men.
Our case involves a 69 year old female that presented with a 6 week history of abdominal discomfort and weight loss. An upper endoscopy showed a blockage at the second portion of the duodenum and the upper gastrointestinal series demonstrated stenosis in the same location. An exploratory laparotomy discovered a mass involving 5 cm of the second portion of the duodenum with wall thickening measuring up to 1.3 cm in thickness. The histological report was muscular hypertrophy with mild eosinophils.
This is the first case reported with such a distinctive isolated involvement of the second part of the duodenum.
INTRODUCTION
Idiopathic muscular hypertrophy of the gastrointestinal tract is a very rare condition of unknown aetiology with no predisposing factors. It mainly involves the oesophagus and there are few cases reported affecting the small bowel.
There have been 25 cases reported in the English literature with this condition, and none in the last 20 years.
The present case is unique on account; entailing an adult woman with an isolated segment of idiopathic muscular hypertrophy of the second part of the duodenum causing gastric outlet obstruction.
CASE REPORT
A 69 year old female, presented with a 6 week history of upper abdominal discomfort, nausea and vomiting symptoms. The patient stated she had lost 10 pounds in the past couple of months. She has a past medical history of sarcoidosis and steroid dependent asthma for the past 2 years.
On physical examination of the abdomen, bowel sounds were present and there was no distension, palpable mass, or tenderness noted.
An upper endoscopy showed distal tertiary esophageal contractions, small sliding hiatal hernia with mild gastroesophageal reflux, and an intestinal obstruction at the level of the second portion of the duodenum. The mucosa was normal with the lumen completely constricted. A CT scan demonstrated distension of the stomach and first portion of the duodenum. An UGI study showed severe stenosis of the second portion of the duodenum.

Upper GI series
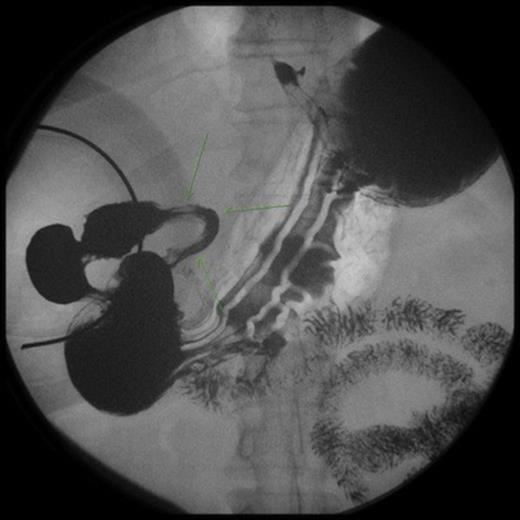
Upper GI series
Upon preparation for surgery, she received pre-operative TPN for 10 days.
An exploratory laparotomy demonstrated an olive type mass in the second portion of the duodenum involving a 5 cm segment of the second portion of the duodenum with thickening of the duodenal wall measuring up to 1.3 cm. A longitudinal duodenotomy showed a diverticulum at the ampulla and two biopsies of the wall were taken. The incision was closed longitudinally and a gastrojejunostomy was performed.
The biopsies reported benign smooth muscle tissue with focal mild increase in eosinophils.
Ten days after the surgery, the duodenostomy dehisced and a roux-en-y duodenojejunostomy was performed. Four hours later, abdominal compartment syndrome was diagnosed, and the patient was taken to the operating room where an abdominal wound VAC for open abdomen was placed. The intestinal function recovered eventually. The skin was closed and after 6 months she returned for fascia closure.
DISCUSSION
This condition is usually asymptomatic. A few patients have described some mild abdominal discomfort (1-3), which was also present with our patient. The most common location of muscular hypertrophy of the gastrointestinal tract in adults is in a short segment of the oesophagus; usually occurring in elderly white men(1).
The first documented record was in 1885 by Reher (1), and the last one in 1988 by Yamagiwa (3). Of which, 18 were adult men between 27 and 74 years old, 2 women of 27 and 68 years, respectively, and 5 children between 9 days and 11 years old. Involvement of the small bowel is even more unusual with only 5 cases published up to date.
All cases involved marked hypertrophy of the muscularis propia (1-4) along with normal mucosa. However, Spencer and Hudson (1) report diverge on a thicker mucosa, and Yamagiwa (3) describes atrophic villi and an extra sheet below the longitudinal layer. Our patient, besides the expected findings, had a focal mild increase in eosinophils.
We conclude that because this is a rare and usually asymptomatic condition, it is very difficult to know what should be the ideal diagnostic test. Nevertheless, if the patient is symptomatic, he/she can be diagnosed with a CT scan and an UGI study or a small bowel series. Depending on the extent of the hypertrophy, the proper treatment may vary. In our opinion, the best possible treatment in this case would have been a Fredet-Ramstedt type myotomy.

{kind=link}
{kind=link}