





Abstract
Schwannomas are rare neoplasms that originate from Schwann cells. We present a case report of schwannoma of the ansa cervicalis in a patient where preoperative imaging suggested thyroid pathology.
A 25-year-old man presented to the otolaryngology department with a one-year history of an asymptomatic, anterior triangle neck swelling. Imaging and FNA suggested a cystic lesion of the thyroid. However, intraoperatively, the lesion was found between the right sternohyoid and thyrohoid and histology showed findings consistent with a diagnosis of schwannoma, determined to originate from the ansa cervicalis based on its anatomical position.
Schwannoma of the ansa cervicalis is extremely rare and there have only been four reported cases in the literature. Schwannomas are often misdiagnosed and confused for other lesions. In our case report we add to the sparse literature on this pathology and highlight common pitfalls in diagnosis and discuss the principles of management of this rare condition.
INTRODUCTION
Schwannomas (also known as neurilemmomas) are rare neoplasms that originate from Schwann cells. They can arise from any peripheral, autonomic, or cranial nerves (with the exception of the olfactory and optic nerves which lack Schwann cells) (1). Between 25-45% of extra cranial schwannomas occur in the head and neck; the majority are benign. We present a case report of the unexpected finding of a schwannoma of the ansa cervicalis in a patient where clinical examination and preoperative imaging suggested a primary thyroid pathology.
CASE REPORT
A 25-year-old man presented to the otolaryngology department with a one-year history of a asymptomatic, anterior triangle neck swelling which he had incidentally noticed. On examination, there was a 3×2cm swelling just right of the midline which moved with swallowing. There was no neck lympadenopathy. The remainder of ENT examination was unremarkable with nasendoscopy showing normal cord movements. Biochemically, he was euthyroid. The general practitioner had organised an ultrasound that showed a 33×26x19mm complex cyst in the right lobe of the thyroid gland. A fine needle aspiration (FNA) was performed and a non-contrast CT scan was requested. The FNA was reported as Thy1; a subsequent ultrasound guided FNA also was reported as Thy1. The CT scan showed a cystic lesion (figure 1) which seemed to be arising from the right lobe of the thyroid gland. Treatment options were discussed and he was listed for a diagnostic right hemithyroidectomy.
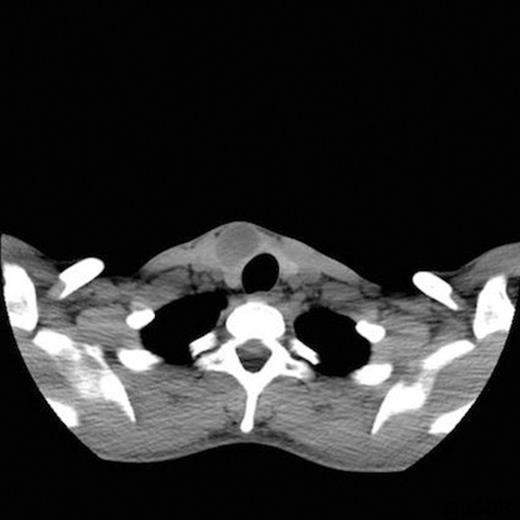
CT scan of schwannoma of ansa cervicalis
Intra-operatively, a cystic lesion was found between the right sternohyoid and thyrohoid muscles. There was no attachment of this lesion to the thyroid gland. Macroscopic findings showed a dull grey fluctuant nodule which on sectioning had a blood filled cavity. Microscopic findings showed fascicles of spindle shaped cells with Verocay bodies consistent with a diagnosis of a schwannoma.
DISCUSSION
Schwannoma of the ansa cervicalis is extremely rare and there have only been four reported cases in the literature. They are notoriously difficult to diagnose as history and clinical examination are non specific. In the head and neck, these tumours are often mistaken for other lesions such as enlarged lymph nodes, carotid body tumours, branchial cysts, or thyroid lesions (2,3). Imaging in the form of CT scan and MRI are helpful in providing some suspicion of a schwannoma (4). On CT, schwannomas appear as well-defined homogeneous masses which show cystic change with contrast enhancement that become more prominent as the lesion enlarges (5). On MRI scans they are well-circumscribed homogenous masses that exhibit high-signal intensity on T2-weighted images and a relatively homogenous low-signal intensity on T1-weighted images. FNA is highly suspicious of schwannoma if spindle cells are isolated. However, diagnosis is only definitively established by histopathological examination of the tumour. This classically shows the pattern of Antoni A and Antoni B cells in addition to Verocay bodies (6).
Complete surgical excision is the treatment of choice as tumours are benign and radio resistant. Incomplete excision may result in slow recurrence over months to years (7).
In our case, preoperative imaging has suggested thyroid pathology therefore the intra-operative findings were unexpected. The preoperative CT did not have contrast enhancement as thyroid malignancy was a differential diagnosis. The blood filled cavity of the lesion was presumably due to the previous FNAs. The position of the schwannoma between the strap muscles was consistent of the nerve of origin being a branch of the ansa cervicalis.
In summary, schwannoma of the ansa cervicalis is rare and is difficult to diagnose preoperatively; our report adds another case to the sparse literature on this pathology.

{kind=link}