





Abstract
A gallbladder incarcerated hernia associated with Mirizzi syndrome is a very rare entity and to our knowledge this is the first case ever described in literature. An 85-year-old man presented at the emergency department with a tender right upper quadrant mass. Computed Tomography (CT) revealed the presence of a gallbladder lithiasis with signs of acute cholecystitis, herniated through the abdominal wall with an associated Mirizzi syndrome. Laparoscopic cholecystectomy and repair of the abdominal wall defect were performed. The patient recovered very well and the postoperative period was uneventful.
INTRODUCTION
Incarcerated gallbladder hernia is an extremely rare condition. Few similar cases are reported in literature but none of them is associated with Mirizzi syndrome. Clinical features are represented by a palpable tender right upper quadrant mass. Radiological images could help the surgeon to choose the surgical strategy and to evaluate the presence of associated diseases. In our case laparoscopic surgery showed to be an excellent approach for both the cholecystectomy and the repair of the defect of the abdominal wall.
CASE PRESENTATION
The patient was an 85 year-old man with history of hypertension, previous surgery for perforated diverticular disease (Hartmann procedure followed by reversal of colostomy). He had suffered from occasional pain in the right upper quadrant for several months. The physical examination showed a 5 cm mass in the right upper quadrant tender to palpation. Ultrasound and CT confirmed the presence of a lithiasic gallbladder herniated through the abdominal wall (fig.1), with a dilatation of the common bile duct that measured 11 mm, due to a 17 mm obstructive infundibular stone as it happens in Mirizzi syndrome type I (fig.2).
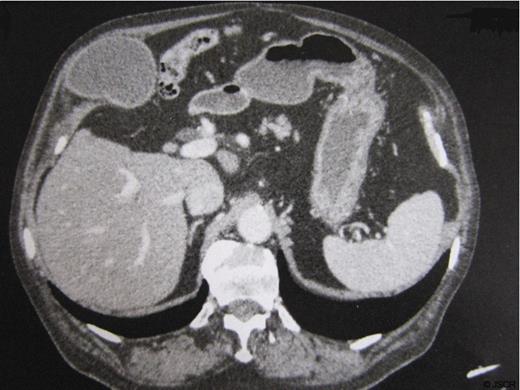
Lithiasic gallbladder herniated through the abdominal wall
The routine complete blood test, including bilirubin level, was unremarkable. Therefore the patient underwent a laparoscopic cholecystectomy and a repair of the hernia. During surgery, multiple adhesions were found and released carefully to identify the gallbladder that was fully included in the right upper quadrant abdominal wall covered by peritoneum. The gallbladder was completely released and the dissection of the pedicle showed a short cystic duct and a normal common bile duct. The cystic duct was dissected and the cholecystectomy completed without inconvenience. The abdominal wall defect was repaired using laparoscopic separated absorbable sutures. The recovery was satisfactory and on the fifth postoperative day the patient was discharged. There were no postoperative complications.

Obstructive infundibular stone
DISCUSSION
The herniation of the gallbladder is an uncommon event. Most of the cases reported in literature are internal hernias through the Winslow foramen (1). The herniation of the gallbladder through acquired defects of the abdominal wall (incisional hernia) has been much less reported. Siriki et al. (2) presented the case of a gallbladder herniated through a fascial defect of a subcostal incision. Garcia reported a patient who presented a gallbladder hernia through a parastomal defect (3). More recently, the case of a gallbladder strangulation through an abdominal wall defect on the site of a previous colostomy was described (4).
In this case, the most remarkable thing is that herniation does not occur through a natural orifice or an acquired defect, such as respectively for the Winslow foramen or for an incisional hernia, but directly into the abdominal wall. To our knowledge, there are only 3 published cases of spontaneous herniation of the gallbladder through the abdominal wall (5,6,7).
Another interesting aspect of this case is the presence of a chronically distended gallbladder (gallbladder hydrops), associated with extrinsic compression of the common hepatic duct by an impacted stone in the infundibulum (Mirizzi syndrome type I) (8). It is probably the gallbladder dilatation that plays an important role in the development of the hernia pressing constantly the gallbladder against the abdominal wall. Usually the clinical picture is represented by a right upper quadrant pain, associated with variable degrees of a compromised general condition. In our experience the preoperative study based on computed tomography is essential for the diagnosis of the gallbladder hernia, and it provides also additional information on the abdominal wall defect.
The management of this type of hernia consists in reducing the content and repairing the abdominal wall defect. In this case the manual reduction was not recommended because of the high risk of gallbladder rupture. We suggest the laparoscopy as surgical approach of first choice because it allows to solve three problems at the same time: first, the reduction of the gallbladder’s incarcerated hernia; second, it enables to perform a cholecystectomy that was indicated for the presence of gallstones and hydrops; third, it allows to repair the hernia defect preferably with a mesh, if the local conditions are favorable.
In our experience, the gallbladder herniation is an ideal indication for laparoscopic surgery.
Preoperative imaging has been proved to detect the gallbladder disease and the morphology of the fascial defect.
Mesh repair is the gold standard for hernias; however, acute cholecystitis still remains a contraindication for mesh repair due to the high risk of infection.

{kind=link}
{kind=link}