





Abstract
The need for intra-operative colonic decompression is commonplace within general surgical theatre. However, cases are usually complex, present late and the risk of perforation with subsequent contamination is high. We describe a novel technique for closed decompression using a laparoscopic trocar and standard pool sucker in a 78-year-old gentleman with an obstructing sigmoid tumour.
INTRODUCTION
Large bowel obstruction and the need for intra-operative decompression is a common problem encountered by many surgeons. High pressure within the loops of bowel predispose to serosal tears and perforation with subsequent contamination of the peritoneal cavity. To avoid such catastrophe, the bowel may be decompressed in situ, this is in itself difficult to achieve without inadvertent spillage of bowel contents into the wound (1). We describe a novel, closed method of decompression using a laparoscopic trocar and a standard pool sucker.
CASE REPORT
A 78-year-old man presented with a history, symptoms and signs of large bowel obstruction, on a background of a longstanding change in bowel habit to a looser stool, bleeding per rectum and recent, absolute constipation. There were also associated symptoms of tenesmus, a poor appetite and weight loss. There was no significant past medical or family history and he was an independent non-smoker. On examination his abdomen was distended with minimal tenderness throughout. There were no masses, hernias or palpable organomegaly but bowel sounds were quiet.
A CT scan was performed which showed a distal colonic stricture causing obstruction at the level of the proximal sigmoid colon. There was also evidence of hepatic metastases and ascites. The large bowel proximal to the stricture was dilated with little gas seen in the small bowel. The most likely diagnosis was a tumour of the sigmoid colon with hepatic metastases. The large bowel was dilated due to a competent ileo-caecal valve.
Laparotomy was performed through a midline incision. On opening the abdomen the loops of large bowel began to balloon from the wound. As the colon was exposed to atmospheric pressure a number of serosal tears appeared spontaneously. The colon contained a large volume of liquid and gas, was friable, and this made it impossible to continue the operation without a risk of spontaneous rupture of the colon. The decision was made to decompress the colon in situ using a closed technique. This would reduce the intra-luminal pressure, allow evacuation of colonic contents and prevent soiling of the wound and the abdomen. This technique would allow the pool sucker to be removed from the bowel and cleaned whenever it became blocked by debris, as often happens in such cases.
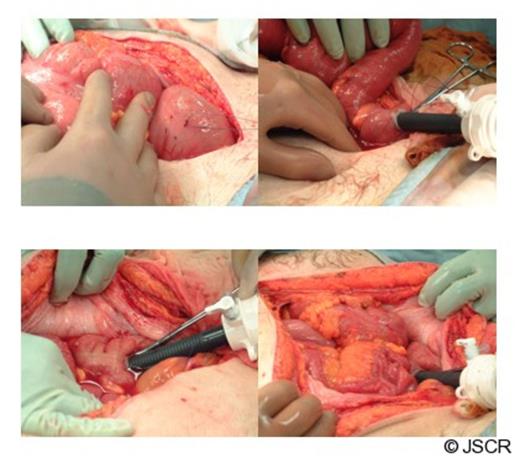
Intra-operative pictures describing the technique
A purse string suture was placed around a tenia coli of the sigmoid colon with a 1.2 cm diameter. A 5/12mm Versaport (covidien TM), ordinarily used for laparoscopic surgery, was inserted through the centre of the purse string suture into the sigmoid colon. This was secured by tightening the purse string suture. A standard pool sucker was inserted through the port into the lumen of the colon and decompression commenced.
With the gas tight seal, it was possible to remove, clean and reinsert the sucker via the Versaport without contaminating the rest of the operating field. With this technique the large bowel was quickly and efficiently decompressed of 3 litres of faecal fluid. Post decompression, a curved clamp was used to isolate the enterotomy and the defect was over sewn.
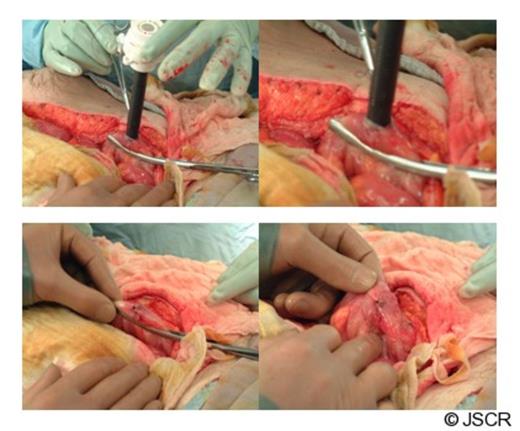
Intra-operative pictures describing the technique
The clamp was removed and there was no contamination of either the wound or the peritoneal cavity. A Hartmann’s procedure was undertaken with resection of an obstructing carcinoma of the sigmoid colon. The patient recovered without any further complication, there was no evidence of either peritonitis or wound infection. He was discharged home on the tenth postoperative day.
DISCUSSION
Closed colonic obstruction is a surgical emergency and may be complicated by spontaneous colonic rupture at the moment of laparotomy, or shortly thereafter as the abdominal compartment is decompressed. It is important that the intra-luminal pressure of the colon is reduced as soon as possible. This may be achieved by the novel application of a laparoscopic port designed to maintain a gas tight seal as instruments are introduced and removed. This case report describes one such method.

{kind=link}
{kind=link}