





Abstract
Portal vein gas is an uncommon ominous radiological sign usually harbouring an intra abdominal catastrophe. When accompanied by pneumatosis intestinalis, it is more predictive of bowel ischemia. We present a case presented with both signs, who suffered from a rare complication of Meckel’s diverticulum.
INTRODUCTION
Portal vein gas is an uncommon ominous radiological sign usually harbouring an intra abdominal catastrophe. We present the case of a 66 years old female presented with acute lower abdominal pain.
CASE REPORT
A 66 years old female presented with acute lower abdominal pain for 2 days. She had a background of hypertension and mesenteric angina. General examination revealed tachycardia and pallor. On abdominal examination, there was tenderness and rigidity in the lower abdomen with signs of peritonitis. Blood results included a CRP of 242, WCC 9.3, mildly elevated urea and creatinine levels, bilirubin 86 and evidence of metabolic acidosis and lactate of 4.2. CT scan revealed intestinal pneumatosis affecting the ileal loops, with free gas in the abdominal cavity and gas in the portal venous system, in keeping with acute ischemia and perforation involving ileal bowel loops (Figure 1 and 2)

CT scan showing portal venous gas and pneumatosis intestinalis in a large intraabdominal cystic mass (Gangrenous Meckel’s Diverticulum)
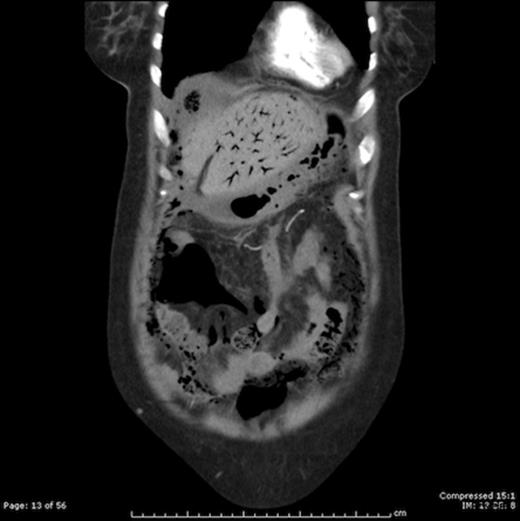
CT scan showing extensive portal venous gas
Laparotomy was performed, and it revealed an infracted and severely necrotic large Meckel’s diverticulum with free fluid in the peritoneal cavity. Limited resection of part of the ileum containing the diverticulum was done. Patient was transferred to the ITU postoperatively. She was in a state of multi-organ dysfunction with a low blood pressure despite being on noreadrenaline support. The liver enzymes were elevated and the platelets’ count was low with elevated prothrombin time. There was oliguria with persistent elevation of the urea and creatinine levels, and the patient eventually needed haemofiltration and required assisted ventilation.
Blood culture revealed Bacteroides Fragilis. Unfortunaetly the patient died with septicaemia and multi-organ failure on the fifth postoperative day.
Pathology reported a 14 cm small bowel loop with large cystic gangrenous lesion arising from the anti-mesenteric surface measuring 10cm at maximum diameter. The orifice of the cyst was circumferentially hypertrophic measuring 3cm in thickness. Microscopic examination revealed ulcerated malignant gastrointestinal stromal tumour (GIST) arising from the orifice of the Meckel’s diverticulum and protruding within the small bowel mucosa.
DISCUSSION
Portal venous gas is a rare radiological sign. It is usually an ominous sign for an underlying intra-abdominal surgical emergency. (1,2) The combination of portal venous gas, pneumatosis intestinalis, and acidosis typically portends bowel ischemia and inevitable necrosis. (3) However, portal venous gas may not predict the severity of the ischemia, which could be reversible. (4) We present a case of acute abdominal emergency with both radiological signs found on CT. The operative findings confirmed a well established gangrene in a large cystic swelling arising from the anti-mesenteric border of the ileum about 60 cm from the ileo-ceacal junction. The cyst was full of necrotic tissue and air. The sign was first Report by Wolfe & Evans in neonates in 1955. (5) It is a rare condition with only 275 cases reported in the literature between 1975 and 2008. (2) Historically, portal venous gas has been associated with high mortality rates and mandatory surgical exploration. The development of the CT uncovered a wide range of pathologies that do not necessarily warrant surgical intervention. (6) This is the reason for the claimed recent decrease in mortality rates, but the rates remain high for cases of bowel ischemia. The case presented, developed multi-organ failure due to the irreversible systemic effect of septicaemia. She died in the ITU on the fifth postoperative day. The radiologic detection of portal venous gas should not then determine the clinical management of the patient; rather the disease severity should. (7)
On the other hand, the risk of neoplasm in a Meckel’s diverticulum is 0.5-5%. Leiomyoma is the most frequent tumor, followed by leiomyosarcoma, carcinoid, and fibroma. GISTs arising from Meckel’s diverticulum are extremely rare; they contribute to 12% of all neoplasm arising in Meckel’s diverticulum. Histo-pathology for the reported case documented a large Meckel’s Diverticulum of 10cm in the greatest diameter with hypertrophied ulcerated malignant gastrointestinal stromal tumour (GIST) at the orifice. (8,9)

{kind=link}
{kind=link}