





Abstract
The incidence of renal cell carcinoma in a pelvic kidney is rare, and has only been described in a very small number of cases. We describe a case where an incidental ectopic kidney with invasive renal cell carcinoma was diagnosed during a separate emergency admission for acute urinary retention.
INTRODUCTION
Renal cell carcinoma is the most common solid tumour occurring within the kidney representing 2-3% of cancers diagnosed. (1) Renal ectopia is also not uncommon and is found in 1 of 2100 to 3000 autopsies (2); however the incidence of renal cell carcinoma in a pelvic kidney is rare, and has only been described in a very small number of cases. (3,4,5)
We describe a case where an incidental ectopic kidney with invasive renal cell carcinoma was diagnosed during an emergency admission.
CASE REPORT
A 55 year old gentleman with a background history of Posterior Cortical Atrophy (PCA) presented with acute urinary retention. He had recently been discharged from a two week respite stay where his wife had noticed one stone of weight loss. He was catheterised and referred onto the admitting surgical team due to high urinary residuals (>1500mls).
This gentleman was constipated but apart from the short history of weight loss and abdominal pain relating to retention, he had no other symptoms. He was haemodynamically stable, with a mild normocytic anaemia (Haemoglobin 12.5g/dL). His urine microscopy subsequently revealed white cells between 107-108 cells/Litre and urine red blood cells >107 cells/Litre.
On abdominal examination, there was a mass palpable in the left iliac fossa, which was initially thought to be an intra-abdominal malignancy and therefore a computed tomography (CT) scan of the abdomen and pelvis was arranged. This demonstrated a normal right kidney, absence of a normally positioned left kidney and a complex solid lobulated 11 x 7 cm mass arising from a presumed left pelvic kidney (Figure 1).
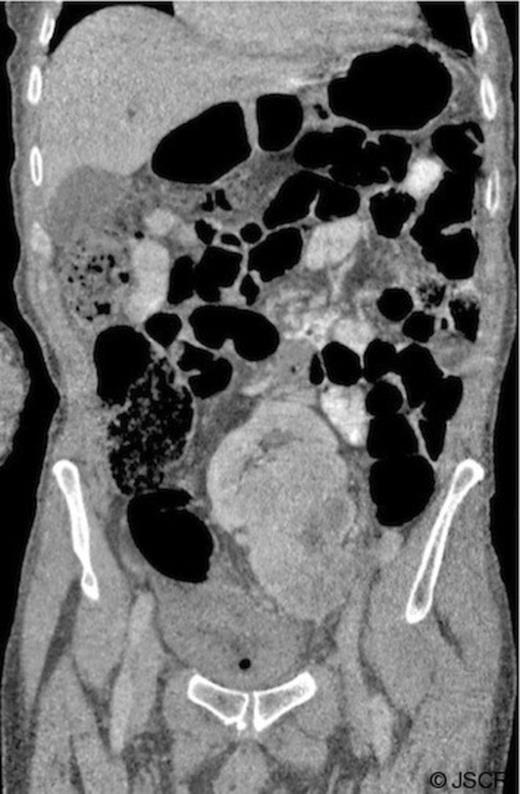
CT of the abdomen and pelvis with oral and intravenous contrast. Coronal image showing a reniform mass in the central pelvis: a presumed left pelvic kidney with a complex heterogenous mass arising and extending inferiorly.
The patient was discharged home with catheter in situ. Following review in the urological outpatient clinic, due to the nature of the patient’s background, the family and clinical team felt that operative management would not be in his best interests and therefore symptomatic management was decided upon. Unfortunately the patient died four months later. A post mortem carried out found a left pelvic kidney infiltrated with a 12cm renal cell carcinoma within the lower pole, with no metastases.
DISCUSSION
Renal ectopia occurs due to mal-ascent of the kidney to the renal fossa. Autopsy series have shown an incidence of the range 1 of 2100 to 3000 autopsies. (1) Most pelvic kidneys are asymptomatic, and there is not thought to be an increased susceptibility to disease. Renal cell carcinoma in a pelvic kidney is extremely rare and has only been documented in a few other cases.
Most cases documented presented with chronic abdominal pain with the pelvic kidney found on ultrasound scan and one case presented with painless haematuria. (4) Our case is the only case documented that was diagnosed whilst presenting with acute urinary retention. This provided an opportunity for a thorough abdominal examination and therefore the abdominal mass was palpated. This case highlights the importance of always performing a full and thorough assessment of a patient, even when they are presenting with a common condition.

{kind=link}