





Abstract
Spigelian hernias are rare, making up only 1-2% of all hernias. Like other hernias, they may contain abdominal contents but are more likely to be incarcerated due to the small size of the fascial defect.(1) We describe here the case of a 71-year-old female with a 10-year history of right lower quadrant pain that remained undiagnosed despite multiple imaging studies. Prior to presentation the patient developed a new bulge and increasing pain at this site; an ultrasound revealed the presence of a bowel-containing hernia. The patient was taken urgently to the operating room for a laparoscopic Spigelian hernia repair, and was found to have an incarcerated appendix in the hernia. After the hernia was reduced, an appendectomy was performed and the hernia was repaired with biological mesh. Postoperatively, the patient did well, and her pain resolved.
INTRODUCTION
Spigelian hernias are rare and often challenging to diagnose. Although many case reports have described the presence of a variety of abdominal organs found in Spigelian hernias, there are no reports of an incarcerated appendix repaired laparoscopically. The use of laparoscopic technique in this case provided easy identification of the incarcerated structure and allowed us to perform an appendectomy without a large incision and with minimal dissection of the abdominal wall.
CASE REPORT
A 71-year-old female presented to our clinic with a 10-year history of right lower quadrant pain. Multiple imaging studies over this time period, including CT and MRI, failed to reveal the etiology of her symptoms. In the week prior to presentation, the patient noticed a new bulge at the site of her chronic pain. An ultrasound demonstrated the presence of a bowel-containing hernia. Examination revealed a non-reducible mass in the right lower quadrant. The patient was taken urgently to the operating room for a laparoscopic Spigelian hernia repair.
Upon laparoscopy, she was found to have an incarcerated appendix in the hernia (Figure 1). After the appendix was carefully reduced, it was noted that the tip of the appendix was necrotic and an appendectomy was performed. The hernia sac was then reduced and excised (Figure 2). The fascial defect was quite small and could be closed in a tension-free manner. Due to the inflammation present and the appendectomy performed, permanent mesh was contraindicated. The hernia was therefore repaired primarily with nonabsorbable monofilament sutures and buttressed with a biological mesh underlay. Postoperatively the patient made good progress and was discharged on postoperative day 5 after return of bowel function. The patient was seen in outpatient clinic twelve days after discharge from the hospital and remains pain-free six months later.
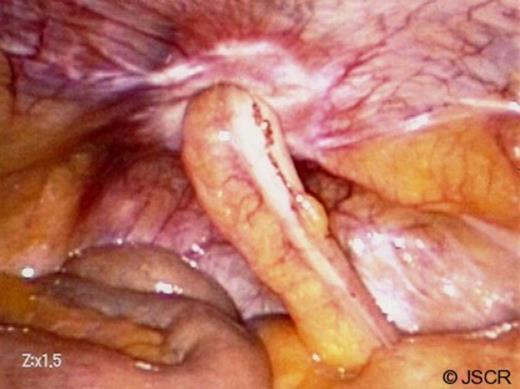
Incarcerated appendix
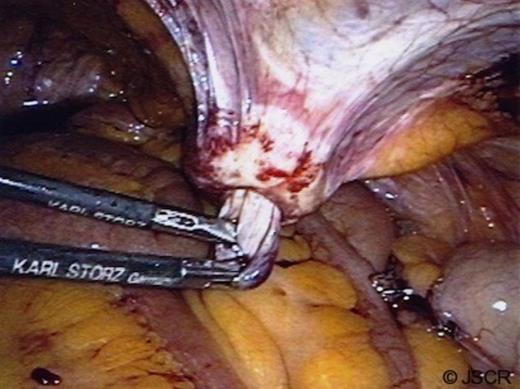
Reduction of the hernia sac
DISCUSSION
The incidence of spigelian hernias is low, but they are the most common type of spontaneous lateral ventral hernia. They are defined by protrusion of the peritoneal sac, an organ, or preperitoneal fat through the Spigelian aponeurosis which is located between the semilunar line laterally and the lateral aspect of the rectus muscle medially. (1) The most common presenting symptoms are pain and the presence of a lump. However, these are notoriously difficult to diagnose on physical exam given that they are often obscured by abdominal fat and the external oblique aponeurosis. (2)
Spigelian hernias can be repaired in a traditional open fashion or laparoscopically, but the basic tenets of hernia repair must be applied in both situations. Laparoscopic repair of spigelian hernias has been shown to be a viable option in the setting of elective repair, although one study recommended extraperitoneal repair in cases in which there is no known incarceration. (3,4) Laparoscopy has also been reported as a method of diagnosis of Spigelian hernias in cases where preoperative workup did not provide a definitive diagnosis. Additionally, the use of laparoscopic repair with mesh has been reported for repair of an incarcerated small bowel. (5)
Multiple intra-abdominal organs have reportedly been found in spigelian hernias, but the presence of an appendix is very rare. (6,7,8) All prior reports of appendix-containing spigelian hernias have repaired the defect using open technique. In this case, the use of intraperitoneal laparoscopy allowed easy identification and subsequent management of the incarcerated appendix with minimal dissection of the abdominal wall structures.

{kind=link}
{kind=link}