





Abstract
Oral pyogenic granuloma (OPG) is a benign vascular proliferation that presents as a solitary, pedunculated, or sessile lesion, associated with irritative factors. Various systemic disorders, particularly type 2 diabetes mellitus (DM2), may contribute to its onset and progression through inflammatory and endothelial mechanisms. This clinical case report describes a 63-year-old male with a history of controlled hypertension and DM2 with glycated hemoglobin (HbA1c) of 7.97%, diagnosed with stage III, grade C generalized periodontitis. Therapeutic management began with periodontal phase I, including personalized oral hygiene instructions and scaling and root planning. After re-evaluation at 5 weeks, an excisional biopsy of the hyperplastic lesion was performed. Histopathological analysis confirmed OPG. The postoperative course was favorable, with proper healing at 15 days. Recent studies indicate that T2DM exacerbates periodontal inflammation through advanced glycation end-products and receptor for advanced glycation end-products (RAGE) signaling, accelerating OPG progression. Multidisciplinary approaches, including glycemic optimization, improve outcomes in these comorbidities.
Introduction
Oral pyogenic granuloma (OPG) is a benign vascular proliferation, usually solitary, pedunculated, or sessile, that occurs on the oral mucosa. It is characterized by its small size and erythematous appearance, with a tendency to ulcerate [1–3]. It is typically asymptomatic or may cause minimal bleeding [3, 4]. This condition is more prevalent in women between the second and fourth decades of life [1, 2].
The most frequent site of oral OPG is the gums, followed by the lips, tongue, buccal mucosa, alveolar ridge, and palate. Although its etiology is not fully understood, several theories have been proposed regarding its onset and development, including a possible infectious component, biofilm and/or dental calculus, trauma, and systemic variations [5–8]. Various metabolic disorders may contribute to the pathophysiology, progression, and recurrence of OPG. Type 2 diabetes mellitus (T2DM) is an important factor, as it is associated with endothelial dysfunction, uncontrolled angiogenesis, oxidative stress, and exacerbation of a chronic inflammatory state [6].
The management of OPG has been widely described in case reports; however, in systemic conditions, especially T2DM linked to periodontal disease, it remains insufficient [6]. The aim of this article is to describe the clinical presentation and therapeutic approach to OPG in a patient with T2DM. This case report was prepared in accordance with the CARE guidelines. The completed CARE checklist is provided as supplementary material.
Case report
A 63-year-old male patient with a history of controlled hypertension and T2DM, was diagnosed with stage III, grade C generalized periodontitis. For high blood pressure, he was prescribed antihypertensive treatment with losartan 50 mg orally every 24 h, managing blood pressure levels of 130/80 mmHg. Regarding the control for T2DM, the patient receives insulin glargine of 10–20 IU subcutaneously at night; laboratory analysis showed a glycosylated hemoglobin (HbA1c) of 7.97%, obtained two days prior to the initial consultation. He presented to the dental clinic complaining, ‘I have problems with my gums. I bite them and they bleed.’
Clinical examination revealed abundant calculus and dental biofilm, edematous and erythematous tissue, and bleeding on probing. An exophytic tissue growth was identified, multilobulated, oval, and fibrous in appearance, located in the mucogingival area, measuring ~1.2 × 0.9 × 0.6 cm. It was erythematous with whitish areas and originated at the base of the papilla and adjacent masticatory mucosa, with a pedunculated base extending toward the interproximal region of teeth 42 and 43 (Fig. 1). The patient reported difficulty chewing. The digital periapical radiograph revealed no relevant findings (Fig. 2).

Clinical characteristics of the lesion. Exophytic lesion located in the mucogingival area measuring ~1.2 × 0.9 × 0.6 cm: It exhibits a predominantly erythematous surface with localized areas of pale pink tissue and superficial whitish zones, suggesting varying degrees of vascularization and possible superficial ulceration. The lesion has a broad pedunculated base and a lobulated surface.
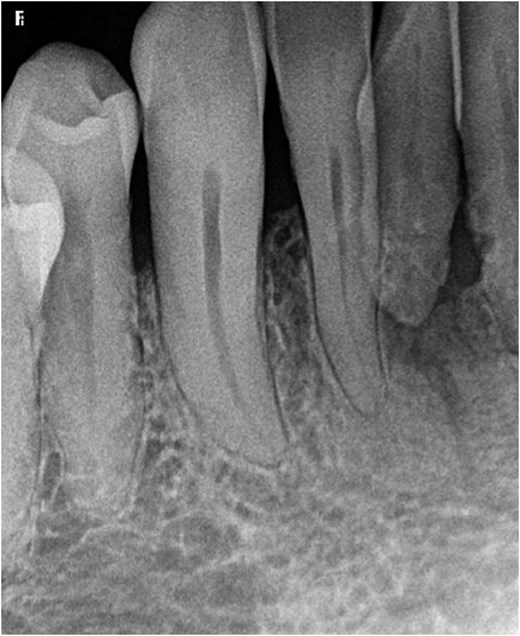
Periapical radiographs corresponding to the location of the lesion. Dental organs show preserved root morphology, continuous lamina dura, and alveolar bone crest within normal limits, with preserved height and contour in relation to the evaluated teeth, without signs of significant horizontal or vertical bone resorption, and without images suggestive of osteolytic lesion or cortical compromise.
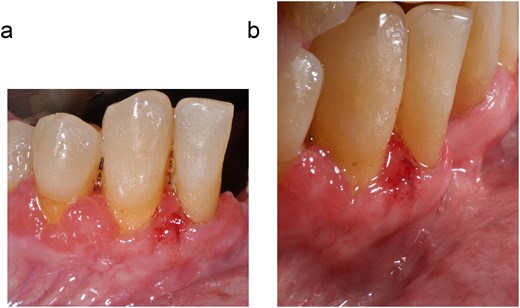
Therapeutic management consisted of several stages. First, periodontal phase I was completed, including personalized oral hygiene instructions and scaling and root planning. After re-evaluation at 5 weeks, an excisional biopsy of the hyperplastic lesion was scheduled (Fig. 3). The surgical procedure involved administering local anesthesia (3% mepivacaine hydrochloride) under aseptic and antiseptic conditions. Using a 15c scalpel blade, resection was performed from the pedunculated base to the interproximal area of teeth 42 and 43, ensuring adequate surgical margins. Bone curettage was then performed. The sample was fixed in 10% formalin and sent to pathology. The site was sutured with simple 6–0 polypropylene monofilament stitches (Fig. 4). Additionally, tooth 41 presented severe bone loss and grade III tooth mobility (Miller classification), which corresponds to a poor periodontal prognosis; consequently, due to the severe destruction of the periodontal support and the zero probability of short-term preservation, the decision was made to carry out the extraction of said tooth in parallel with the surgical intervention of the excisional biopsy of the entity. Amoxicillin 750 mg every 12 h for 7 days, ibuprofen 600 mg every 8 h for pain, and rinses with 0.12% chlorhexidine digluconate for 15 days were prescribed. Histopathological analysis confirmed the diagnosis of OPG (Fig. 5).
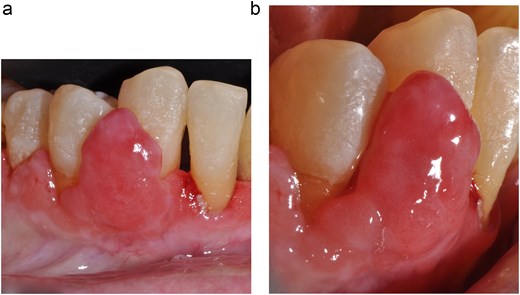
(a and b) Clinical checkup 5 weeks after removal of local irritants. Exophytic lesion with evident reduction in size. The previous intense erythema has diminished, with a more homogeneous reddish-pink coloration and less superficial hemorrhagic component. The surface appears smoother and shinier, without extensive areas of active ulceration. The adjacent gingival tissues show improvement in the inflammatory component, with reduced marginal edema following periodontal phase I. No clinical signs of underlying bone involvement are apparent. The partial reduction in size after removal of the irritant factor is consistent with the reactive behavior of the lesion and its dependence on local stimuli.
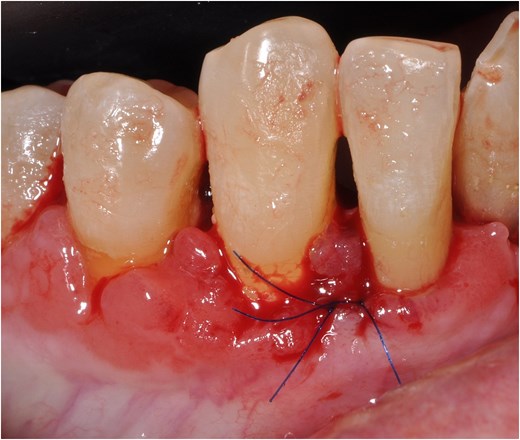
Immediate postoperative period following surgical excision. The surgical bed immediately after complete excision of the lesion shows regular margins, with remaining gingival tissue that is erythematous and slightly edematous, consistent with recent surgical trauma. Simple 6–0 polypropylene monofilament sutures were used.
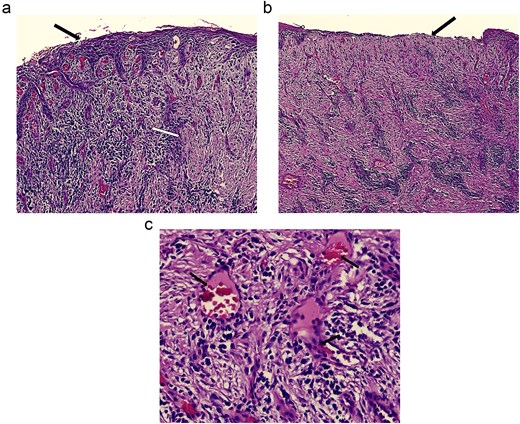
Photomicrographs stained with Hematoxylin and Eosin, corresponding to the histopathological study. (a) The lesion is covered by parakeratinized stratified squamous epithelium, which exhibits atrophy, leukocyte migration, and inter- and extracellular edema (black arrow). Beneath the epithelium, loose fibroconnective tissue is observed with mild interstitial edema, blood capillaries, and a moderate diffuse inflammatory infiltrate (white arrow) (10×). (b) In one field, the lesion shows loss of epithelial continuity consistent with an ulcer (black arrow) (10×). (c) The lesion consists of granulation tissue hyperplasia. Numerous congested blood capillaries (black arrows), fibroblasts, loose collagen fibers, and a diffuse, severe mixed inflammatory infiltrate composed of lymphocytes, plasma cells, and neutrophils are observed (40×).
At the 15-day follow-up, adequate healing was evident. The sutures were removed without signs of inflammation, infection, or complications (Figs 6 and 7).
(a and b) Clinical images at the 15-day follow-up after excisional biopsy. The postoperative course was satisfactory 15 days after excision of the lesion, with suture removal and no signs of inflammation, infection, or complications. Adequate healing was observed. Additionally, tooth #41 was extracted, and the socket is in an advanced stage of healing. The adjacent gingival margins show a more homogeneous pink-coral coloration, with a notable reduction in erythema and edema compared to the immediate postoperative period.

Periapical radiograph taken 15 days after excisional biopsy and tooth extraction. Radiographic findings are similar to the initial radiograph. The absence of tooth 41 is evident, showing the edentulous space. The alveolar socket shows a regular contour, a homogeneous trabecular pattern undergoing reorganization, and continuous cortical bone, without residual radiolucent images suggestive of a persistent periapical lesion.
Discussion
OPG is considered one of the most common reactive entities with a higher prevalence in the gingivae, highlighting the importance of periodontal condition in its progression [2, 8]. In this clinical case, the coexistence of stage III, grade C generalized periodontitis and T2DM with suboptimal glycemic control (HbA1c 7.97%) creates a favorable environment for exacerbated inflammatory and vasoproliferative responses.
Dental calculus and biofilm are decisive factors in promoting a persistent immunoinflammatory state, leading to cytokine production that favors fibroblastic proliferation and neoangiogenesis, resulting in the growth of vascularized connective tissue [8]. In the clinical context of T2DM with suboptimal glycemic control (HbA1c 7.97%), this proliferation is further intensified by the persistent accumulation of advanced glycation end products (AGEs), whose binding to RAGE receptors promotes proinflammatory signals, increases oxidative stress, and compromises endothelial function. Given this inflammatory and proangiogenic scenario, the OPG progression intensifies [6]. In this case, the objective metabolic findings (HbA1c 7.97%) emphasize that glycemic imbalance contributed significantly to the clinically identified proinflammatory and proangiogenic environment, highlighting the association between poor metabolic control and the exacerbated presentation of oral inflammatory entities.
Surgical excision with a scalpel is the conventional treatment, typically providing effective resolution in a single procedure, as was the therapeutic approach in this case [8, 9]. However, new complementary therapeutic approaches have been proposed, such as diode laser, curettage, cryotherapy with liquid nitrogen, or sclerotherapy, which have shown some benefit in treatment without significant complications for the patient [10–13]. Despite this, current evidence remains limited, and further research is needed to determine whether these strategies are more effective than conventional treatment, or whether combining different treatments can reduce recurrence, particularly in patients with T2DM.
Conclusion
Integrated management of oral OPG in T2DM involves eliminating etiological factors through initial periodontal therapy, followed by surgical excision of the lesion and site conditioning to promote optimal healing. This case highlights OPG as resulting from the interaction between local irritants, such as biofilm and calculus, and systemic dysregulation in T2DM, including AGE-RAGE-mediated inflammation, oxidative stress, and endothelial dysfunction, which enhance vasoproliferative responses.
Therapeutic success depends on multidisciplinary coordination, strict glycemic control (e.g. HbA1c <7%), and regular monitoring to reduce recurrence. The active participation of oral pathologists, periodontists, internists, and nutrition professionals allows for comprehensive management for treatment and reduction of the risk of recurrence. Although non-surgical periodontal therapy may help improve metabolic control, the literature supports that the impact on HbA1c is limited, with decreases of values close to 0.5% in 12 months [14]. Consequently, periodontal management is a complementary element considered in a comprehensive strategy that incorporates optimization of medical treatment, pharmacological adherence, nutritional adjustment, and periodic monitoring to achieve the most favorable HbA1c parameters.
Emerging modalities such as diode laser and cryotherapy require further evaluation for efficacy in T2DM populations and may reduce invasiveness. The bidirectional relationship between T2DM and periodontitis underscores the importance of non-surgical periodontal interventions for improving glycemic control and resolving lesions. Longitudinal studies are needed to validate the impact of combined therapies on recurrence rates in patients with comorbid conditions.
Author contributions
Francisco Javier Alcaraz-Baturoni (Writing—review and editing, Writing—original draft preparation, Visualization, Validation, Supervision, Methodology, Formal analysis, Conceptualization), Jessica Paola Ibarra-González (Writing—review and editing, Writing—original draft preparation, Visualization, Validation, Supervision, Methodology, Formal analysis, Conceptualization), Luis Fernando López-Hernández (Writing—review and editing, Writing—original draft preparation, Visualization, Validation, Supervision, Formal analysis, Conceptualization), Mario Alberto Alarcón-Sánchez (Writing—review and editing, Writing—original draft preparation, Visualization, Validation, Supervision, Formal analysis, Conceptualization), Daniel Ortuño-Sahagún (Writing—review and editing, Writing—original draft preparation, Visualization, Validation, Supervision, Formal analysis, Conceptualization), Artak Heboyan (Writing—review and editing, Writing—original draft preparation, Visualization, Validation, Supervision, Formal analysis, Conceptualization), Juan Pablo González-Cárdenas (Writing—review and editing, Writing—original draft preparation, Visualization, Validation, Supervision, Formal analysis, Conceptualization), and Sarah Monserrat Lomelí-Martínez (Writing—review and editing, Writing—original draft preparation, Visualization, Validation, Supervision, Methodology, Formal analysis, Conceptualization)
Conflicts of interest
All authors report no relevant conflicts of interest for this article.
Funding
None declared.
Data availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Patient informed consent
The study participant provided informed written consent prior to study enrollment.
CARE checklist (2016) statement
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}