





Abstract
Bouveret syndrome is an uncommon form of gallstone ileus that results from a cholecystoenteric fistula. Impaction of gallstone in the proximal duodenum blocks the gastric outlet. We report the first case from a resource-limited setting. A 75-year-old man with calculous cholecystitis arrived with gastric obstruction, melena, coffee-ground emesis, and weight loss. Lab data showed leukocytosis and mild anemia. Computed tomography scan showed gastric distension, pneumobilia, and a gallstone in the duodenum: the characteristic findings in Rigler’s triad. Due to its large size and calcification, endoscopic extraction was unsuccessful, and this necessitated surgical enterolithotomy. Despite the technical success of the surgery, the patient passed away two days later due to heart arrhythmia. This case report highlights the necessity of prompt surgical intervention when modern endoscopic alternatives are not accessible.
Introduction
A cholecystoenteric fistula, secondary to chronic cholecystitis, allows gallstones to migrate, causing intestinal obstruction. Computed tomography (CT) is helpful ascertaining the correct diagnosis, particularly when symptoms resemble peptic ulcer disease [1]. Failure of endoscopic extraction often necessitates surgical enterolithotomy, especially in resource-limited settings where advanced lithotripsy techniques are not available [2]. We present the first documented case of Bouveret syndrome from a resource-limited healthcare system to illustrate the therapeutic challenges encountered after failed endoscopic extraction and the complexities of surgical decision-making in an elderly patient with multiple comorbidities.
Case presentation
A 75-year-old man presented with a three-day history of recurrent coffee-ground emesis and melena. There was no history of frank hematemesis or hematochezia. He also reported unintentional weight loss and reduced oral intake. In addition, he had not passed stool or flatus for 2 days.
He had ischemic heart disease, type 2 diabetes mellitus, and a history of inguinal hernia repair. He had been treated conservatively for calculous cholecystitis one month prior. Aspirin 81 mg once day, bisoprolol 2.5 mg once daily, omeprazole 40 mg once daily, metformin 1000 mg once daily, and vildagliptin 50 mg once daily were among his usual medications.
On admission, he was tachycardic at 105 beats per minute but remained normotensive, consistent with a compensated hemodynamic state. Chest examination revealed fine bilateral basal crackles. The abdomen was soft and non-tender, with no palpable organomegaly. Plain abdominal radiography was non-diagnostic. Laboratory investigations revealed mild leukocytosis (12 000/mm3; normal up to 10 000/mm3), mild anemia (hemoglobin 10 g/dl; normal: 12–16 g/dl), and hyperglycemia (140 mg/dl; normal: 108 mg/dl). Renal function, electrolyte levels, and other biochemical parameters were within normal limits. Preoperative electrocardiography and electrocardiography showed no acute abnormalities.
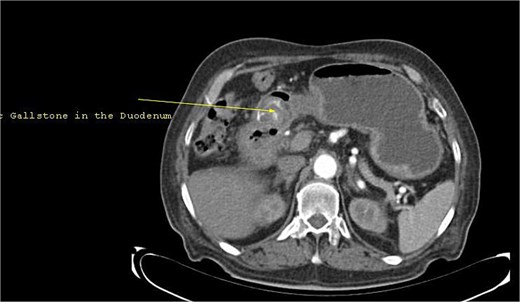
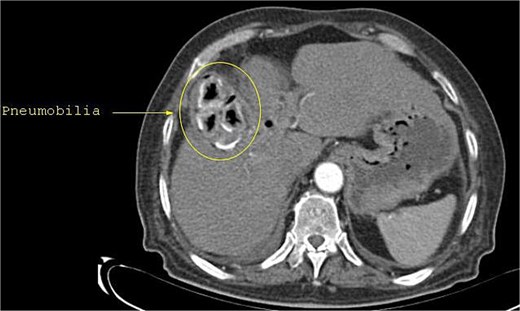
Initial upper gastrointestinal endoscopy was limited by retained coffee-ground material obscuring visualization of the gastric mucosa. Following gastric lavage, a large gallstone was identified impacted within the pyloric channel (Fig. 1). Subsequent CT confirmed the presence of pneumobilia (Fig. 2), marked gastric distension (Fig. 3), and an ectopic gallstone within the proximal small bowel (Fig. 4), findings consistent with Rigler’s triad [3]. These findings were consistent with Bouveret syndrome causing gastric outlet obstruction [1].
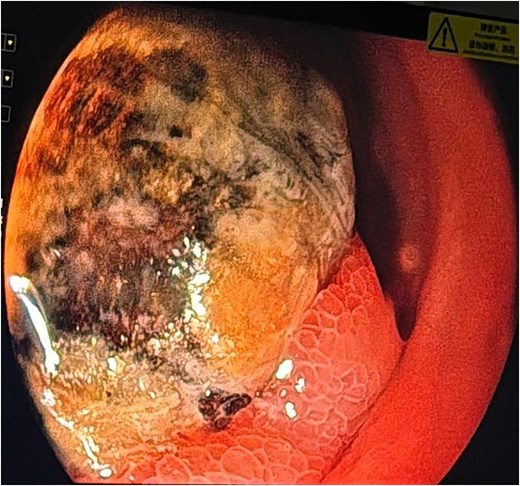
Gallstone in the duodenal bulb with gastric outlet obstruction.
Abdominal CT revealing pneumobilia, characterized by branching radiolucent tracts within the intrahepatic biliary tree.
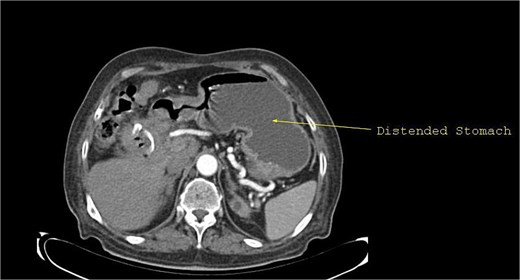
CT demonstrating marked gastric distension secondary to mechanical obstruction at the duodenal bulb.
CT revealing an ectopic gallstone within the proximal small bowel.
Initial management focused on intravenous fluid resuscitation and proton pump inhibitor therapy. Endoscopic retrieval failed because of the large size and firm impaction of the stone, while advanced lithotripsy techniques were unavailable. The patient therefore underwent open surgical exploration. Intraoperative findings revealed a markedly inflamed gallbladder containing multiple residual gallstones, a large cholecystoduodenal fistula, and additional duodenal calculi, including a large, impacted stone causing gastric outlet obstruction. Based on these findings, enterolithotomy, cholecystectomy, and fistula repair were performed. No significant intraoperative blood loss or surgical complications occurred [4]. The immediate postoperative course was initially stable; however, the patient subsequently developed ventricular fibrillation and died two days after surgery despite resuscitative measures.
Discussion
Bouveret syndrome is a rare cause of gastric outlet obstruction resulting from impaction of a gallstone in the pylorus or proximal duodenum after formation of a cholecystoenteric fistula. It typically arises in the context of long-standing cholelithiasis and recurrent cholecystitis, where chronic inflammation leads to adhesion and erosion between the gallbladder and adjacent gastrointestinal tract, allowing passage of a large gallstone into the upper digestive tract [1, 2, 4].
Most affected are elderly with comorbidities; chronic inflammation and reduced reserve cause delayed, nonspecific presentation mimicking other gastrointestinal diseases [1].
Prolonged stone impaction may cause mucosal ischemia and ulceration, resulting in upper gastrointestinal bleeding and potentially obscuring the diagnosis [5].
CT is the imaging modality of choice, demonstrating pneumobilia, an ectopic gallstone, and proximal gastrointestinal dilatation, classically described as Rigler’s triad. However, all three components are not always present, particularly in early disease, and diagnostic sensitivity varies with disease stage and fistula maturity [4, 6].
Endoscopy may be both diagnostic and therapeutic, but its success is often limited. Large, impacted gallstones are frequently not amenable to retrieval with standard devices due to size, hardness, and unfavorable angulation. In addition, retained gastric contents may obscure visualization [4]. Reported success rates of endoscopic extraction remain low, and advanced lithotripsy techniques are not universally available, particularly in resource-limited settings.
When endoscopic therapy fails, surgical intervention is required [2, 7].
Although enterolithotomy alone is often preferred in elderly high-risk patients to reduce operative stress, definitive surgery with cholecystectomy and fistula repair may still be required depending on intraoperative findings and resource availability. In resource-limited settings where advanced endoscopic and postoperative support are restricted, single-stage surgery may be selected despite increased perioperative risk [8]. Spontaneous fistula closure may occur, and recurrence is uncommon. Reported morbidity and mortality remain significant due to advanced age and comorbidities [9].
When endoscopic therapy fails, surgery is required. Enterolithotomy alone is generally favored in elderly patients with substantial comorbidity because it reduces operative duration and physiological stress [8–10]. In our patient, however, intraoperative findings demonstrated a markedly inflamed gallbladder containing multiple residual gallstones, a large cholecystoduodenal fistula, and additional duodenal calculi. These findings influenced the decision to perform cholecystectomy and fistula repair in addition to stone extraction. Although no significant blood loss or intraoperative complications occurred, the possibility that the greater operative burden contributed to the subsequent fatal ventricular arrhythmia cannot be excluded.
The optimal surgical approach in Bouveret syndrome remains controversial. Enterolithotomy alone is generally favored in elderly patients with substantial comorbidity because it shortens operative duration and reduces physiological stress. However, our patient had a markedly inflamed gallbladder containing multiple residual calculi and a large cholecystoduodenal fistula identified intraoperatively. These findings influenced the decision to proceed with definitive surgery, including cholecystectomy and fistula repair. Although the operation was completed without significant blood loss or intraoperative complications, the possibility that the increased operative burden contributed to the subsequent fatal ventricular arrhythmia cannot be excluded. This case highlights the importance of individualized operative decision-making when balancing definitive treatment against perioperative risk in frail patients.
Conflicts of interest
None declared.
Funding
None declared.
Ethical approval
This case report did not require review by the Ethics Committee.
Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Guarantor
All authors have read and approved the manuscript. The corresponding author acts as guarantor.
References
Turner AR, Kudaravalli P, Al-Musawi JH et al. Bouveret Syndrome (Bilioduodenal Fistula). In:
Turner AR, Sharma B, Mukherjee S. Gallstone ileus. In:
Inukai K. Gallstone ileus: a review.

{kind=link}
{kind=link}
{kind=link}
{kind=link}