





Abstract
Pyogenic granuloma (PG) is a benign vascular lesion of the oral mucosa whose progression is strongly linked to pregnancy, due to increased hormone levels (estrogen and progesterone), which promote an exacerbated inflammatory response. There is controversy regarding the appropriate timing of PG treatment during pregnancy. This clinical case describes a 25-year-old patient, 12 weeks into her pregnancy, who presented with an exophytic, oval, fibrous lesion located on the interproximal gingiva between teeth 32 and 33. Treatment included an initial phase of scaling, coronal and root planing, and oral hygiene instructions; in the second phase, an excisional biopsy was performed. Histopathological findings confirmed the diagnosis of PG. At the 20-day follow-up, proper healing was evident. This case suggests that elimination of local irritating factors is an important component of management; furthermore, an interdisciplinary approach would promote an optimal outcome.
Introduction
Pyogenic granuloma (PG) is a benign, exophytic vascular lesion of the oral mucosa, occurring on a pedunculated or sessile base [1, 2]. Although its etiopathogenesis is not fully established, in the context of pregnancy, increased levels of estrogen and progesterone promote an exacerbated gingival inflammatory response to local irritants, leading to the development of PG in the oral cavity [3, 4].
The clinical significance of oral PG lies in establishing a differential diagnosis, as it may present with clinical features similar to those of other oral lesions [2, 3]. When it occurs during pregnancy, there is controversy regarding the timing of treatment initiation, as some authors assert that expectant management until postpartum is ideal in these patients due to the possibility of spontaneous regression of the lesion [5]; while other authors suggest surgical excision at the time of diagnosis, especially in symptomatic cases or those with rapid growth [6]. The objective of this article is to describe the clinical, histopathological, and therapeutic findings in a patient diagnosed with oral PG in order to guide decision-making in the context of this condition.
Case report
A 25-year-old female patient, 12 weeks pregnant, presented to the dental clinic complaining of swollen gingiva and mild discomfort when chewing. She had no significant medical history, and she did not report any systemic conditions.
On clinical examination, a moderate-to-heavy accumulation of dental biofilm was observed, additionally, erythematous gingival tissue and bleeding on probing were found. An oval, fibrous, exophytic tissue mass measuring ~0.6 × 0.6 cm was present in the vestibular and interdental areas; it was erythematous in color with slightly whitish areas. It had a pedunculated base extending toward the interproximal region of teeth 32 and 33 (Fig. 1). The digital periapical radiograph revealed no significant findings.

Clinical image of exophytic tissue growth in attached gingiva, oval-shaped, fibrous, and erythematous.
The therapeutic management consisted of several stages. In phase I, scaling and root planning were performed, along with personalized oral hygiene instructions. Phase II consisted of performing an excisional biopsy of the hyperplastic lesion. The surgical procedure was performed under aseptic and antiseptic conditions, and local anesthesia (2% lidocaine) was administered. Using a No. 15c scalpel blade, the lesion was removed from the pedunculated base to the interproximal area of teeth 32 and 33, ensuring proper surgical margins; bone curettage was then performed. The biopsy specimen was placed in 10% formalin and sent for histopathological examination (Fig. 2). The site was sutured with 6–0 polypropylene monofilament simple sutures.
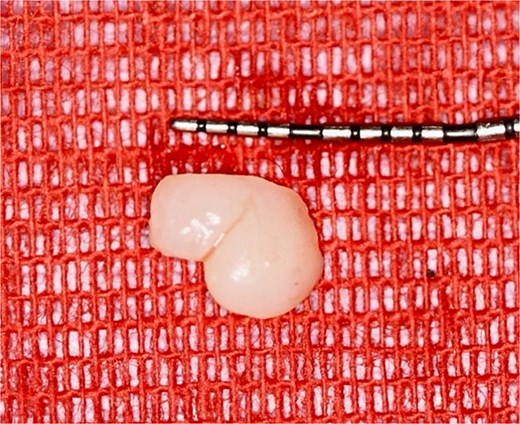
Surgical specimen after excision of the exophytic lesion.
For postoperative management, although no clinical signs of active infection were present at the time of the procedure, amoxicillin 750 mg was prescribed every 12 h for 7 days as a prophylactic purpose based on clinical judgment. This was due to the gingival inflammation in the lesion area related to the accumulation of dental biofilm and because the procedure involved surgical excision followed by curettage of the surgical site. Additionally, paracetamol 500 mg was recommended every 8 h only for pain, and 0.12% chlorhexidine digluconate mouthwash was prescribed for 15 days. Histopathological analysis confirmed an oral PG (Fig. 3a–d).
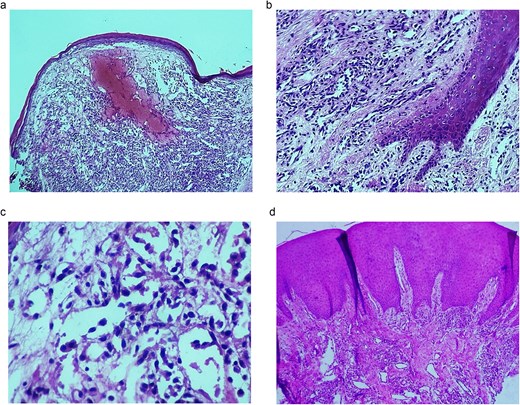
(a) Photomicrograph 10×: A lobular lesion is observed, its surface composed of keratinizing stratified squamous epithelium with flattening of the rete ridges. Beneath the epithelium, a lesion is characterized by proliferation of abundant capillaries over a myxoid stroma with a central focus of hemorrhage. (b) Photomicrograph 40×: On the left of the image, squamous epithelium corresponding to an epithelial collarette can be seen. (c) Photomicrograph 40×: The capillaries show edematous-looking endothelial cells with polymorphic nuclei of fine chromatin on small eosinophilic cytoplasms. (d) 4× photomicrograph: Panoramic image showing mucosa peripheral to a lesion with stratified squamous epithelium.
At the 20-day follow-up, proper healing was observed. The sutures were removed without signs of infection, inflammation, or complications.
The patient expressed fear of the treatment, especially regarding the use of anesthetic and medications, as well as the possibility of bleeding, since this could endanger the fetus. However, after receiving clear and concise information about the procedure, postoperative care, and follow-up management, she said she felt calmer. After the procedure, she experienced only mild discomfort, without any significant complications. She expressed satisfaction with the care she received throughout her treatment.
Discussion
During pregnancy, ~3% of patients will experience an episode of oral PG [7]. The site with the highest incidence is the gingiva in the anterior region of the maxilla [2]. It is typically more common in the first trimester, particularly between the second and third months of pregnancy, due to the progressive increase in estrogen and progesterone characteristic of pregnancy [8–11].
During the early follicular phase, follicle-stimulating hormone (FSH) induces the development of multiple ovarian follicles, which secrete estrogen into the systemic circulation until one follicle becomes dominant. The secreted estrogen acts via a negative feedback mechanism at the pituitary level, decreasing the release of FSH [4]. The dominant follicle grows until it finally ruptures, resulting in ovulation. If fertilization occurs, progesterone and estrogen levels progressively increase, supporting pregnancy viability. Estrogens, and to a lesser extent progesterone, act on the endothelium of the body’s microvasculature in a physiological manner, facilitating the growth and development of the fetoplacental unit, angiogenesis, and trophoblastic invasion into the basal decidua, and increasing vascular permeability [12–14]. These effects are mediated by the release of various factors, notably vascular endothelial growth factor (VEGF), fibroblast growth factor (FGF), placental growth factor, tumor necrosis factor α (TNF-α), and hypoxia-inducible factor (HIF) [13].
VEGF acts as a potent mitogen for endothelial cells, promoting angiogenesis and increasing vascular permeability. FGF, on the other hand, comprises a large family of proteins expressed primarily in macrophages and mast cells, with multiple functions, including angiogenesis, granulation tissue formation, and embryonic development. Furthermore, HIF is a protein expressed only under hypoxic conditions, inducing angiogenesis through the stimulation of VEGF, thereby promoting the neovascularization cycle [8]. The development of PG is not related to a specific mechanism; rather, it is the result of exposure to multiple causative factors leading to the lesion’s onset. It has been proposed that chronic irritation of the gingival tissue or local trauma to the gingiva constitutes the initial stimulus, from which granulation tissue and angiogenesis form via macrophages and endothelial cells that secrete VEGF, FGF, and HIF to repair the disruption of periodontal tissue continuity [1, 2]. In this context, the excess of hormones characteristic of pregnancy promotes an exaggerated granulation tissue response and serves as a potent positive feedback stimulus for VEGF secretion, favoring the development of the lesion and the formation of new blood vessels [2]. Similarly, progesterone increases susceptibility to local mechanical irritants. Furthermore, the accumulation of dental biofilm promotes dysregulation of the immune system in response to the wound, intensifying the inflammatory response and gingival hyperplasia. As a final result, an inflammatory, erythematous, and frequently painful vascular lesion develops (Fig. 4) [9, 11].
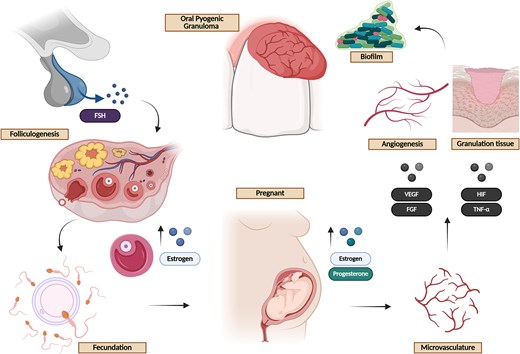
Pathophysiological sequence of the development of oral pyogenic granuloma during pregnancy. Follicle-stimulating hormone (FSH) induces the growth of ovarian follicles, which secrete estrogens; following ovulation and in the event of fertilization, levels of estrogen and progesterone gradually increase. These hormones act on the microvasculature, promoting the release of proangiogenic mediators such as vascular endothelial growth factor (VEGF), fibroblast growth factor (FGF), and hypoxia-inducible factor (HIF). In the presence of local irritative stimuli, such as dental biofilm, food impaction, or mechanical trauma, an inflammatory response is triggered that promotes the formation of granulation tissue and angiogenesis. The hormonal environment of pregnancy enhances this response, increasing vascular permeability and tissue proliferation, which culminates in the formation of a characteristic inflammatory vascular lesion, clinically consistent with pyogenic granuloma created in BioRender. (2026) https://BioRender.com/d34u8o5.
The conventional treatment for PG involves surgical excision of the lesion, along with oral hygiene measures and the elimination of local irritants [2]. However, in the context of pregnancy, the therapeutic approach remains a subject of debate. Because the lesion is highly vascularized, surgical intervention may be associated with profuse bleeding; therefore, its removal is usually reserved for certain cases. For this reason, during pregnancy, expectant management is preferred, controlling the causative factors through proper oral hygiene and periodic follow-up to assess the lesion’s progression [14, 15]. Generally, the main indications for surgical management are uncontrolled heavy bleeding, significant pain, or when the lesion interferes with masticatory function. In the present case, this management of the entity was selected because it generated mild discomfort and manifested in an area of dental biofilm retention and persistent irritation; likewise, a histopathological confirmation was necessary; allowing a diagnostic and therapeutic approach, in addition to periodontal therapy. Other therapeutic approaches include cryotherapy, laser excision, electrosurgery, or partial tissue removal; however, the latter approach is usually associated with high recurrence rates [2].
Following surgical excision, the recurrence rate can reach up to 20% of patients [2]. This has been associated with incomplete removal of the tissue at the time of surgical excision, as well as the persistence of causative factors, such as biofilm or gingival trauma, and the emergence of new lesions in the gingival mucosa [1, 2, 11]. In this regard, controlling these factors is essential regardless of the treatment used; therefore, strict clinical monitoring is recommended, focused on maintaining oral hygiene through the removal of dental biofilm and the regular use of dental floss, with the aim of preventing recurrence and eliminating causal factors that may influence the growth of the lesion.
This clinical case should be interpreted considering some limitations. First, the findings cannot be generalized to other pregnant women with oral progesterone because it is only one reported case. Second, it is impossible to establish causal relationships or consider the implemented treatment superior to other options, given its descriptive nature. Third, the patient was followed for 20 days, so only early healing was evaluated; however, a longer follow-up period is required to consider the recurrence of the lesion, which occurs in up to 20% of cases. Additionally, it was not possible to analyze the effect of hormonal changes in the postpartum period on the evolution of the affected area, as there was no follow-up during this stage. Finally, prospective studies with a representative number of patients are needed to establish more specific indications for postoperative management and findings from the surgical management of the lesion during pregnancy.
Conclusion
Oral PG during pregnancy results from an inflammatory response exacerbated by elevated hormone levels in response to local irritants. Although there is no clear consensus on the optimal timing for therapeutic management, this case demonstrates that timely surgical removal combined with control of local irritants was effective in this patient; in particular, it should be considered when spontaneous bleeding or masticatory interference occurs. To ensure adequate resolution without recurrence of the condition, it is essential to completely remove the lesion, maintain consistent oral hygiene, and address it through an interdisciplinary approach.
Author contributions
Mario Alberto Alarcón-Sánchez (Writing—review and editing, Writing—original draft preparation, Visualization, Validation, Supervision, Software, Resources, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization), Juan Pablo González-Cárdenas (Writing—review and editing, Writing—original draft preparation, Visualization, Validation, Supervision, Methodology, Formal analysis, Conceptualization), Eder Javier Martínez-González (Writing—review and editing, Writing—original draft preparation, Visualization, Validation, Supervision, Methodology, Formal analysis, Conceptualization), Gustavo Eder González-Alvarez (Writing—review and editing, Writing—original draft preparation, Visualization, Validation, Supervision, Methodology, Formal analysis, Conceptualization), Giovanna Victory-Rodríguez (Writing—review and editing, Writing—original draft preparation, Visualization, Validation, Supervision, Resources, Methodology, Investigation, Formal analysis, Data curation, Conceptualization), Artak Heboyan (Writing—review and editing, Writing—original draft preparation, Visualization, Validation, Supervision, Software, Resources, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization), and Sarah Monserrat Lomelí-Martínez (Writing—review and editing, Writing—original draft preparation, Visualization, Validation, Supervision, Methodology, Formal analysis, Conceptualization)
Conflicts of interest
All authors report no relevant conflicts of interest for this article.
Funding
None declared.
Data availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Patient informed consent
The study participant provided informed written consent prior to study enrollment.
CARE checklist (2016) statement
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).

{kind=link}
{kind=link}
{kind=link}
{kind=link}