





Abstract
Adult colonic intussusception caused by lipoma is rarely seen in clinical practice. Due to its infrequency, it is often incidentally diagnosed radiologically in patients presenting with abdominal pain. The challenge of pre-operative diagnosis lies in distinguishing benign lead points such as lipomas from malignant tumours, given that colonic intussusception carries a high risk of underlying malignancy. Urgent diagnosis is therefore essential to exclude a malignant cause and guide appropriate surgical management. We describe a case of a transverse colo-colic intussusception in a 50-year-old female secondary to a histologically confirmed lipoma as the lead point. The patient underwent a right hemi-colectomy and recovered well post-operatively. This case emphasizes the importance of considering intussusception in adults with abdominal pain and highlights that, rarely, they may be caused by benign colonic lesions.
Introduction
Intussusception is the telescoping of a proximal bowel segment into a distal segment. It is rare in adults, accounting for 1%–5% of bowel obstructions [1]. Unlike in children, adult intussusception is commonly caused by a pathological lead point, including inflammatory diseases, adhesions, and tumours [2, 3]. We describe a rare case of an adult female presenting to hospital with abdominal pain who was diagnosed with colo-colic intussusception from a colonic lipoma.
Case presentation
A 50-year-old Caucasian female presented to a metropolitan emergency department with a 24-hour history of generalized crampy abdominal pain and associated nausea. She reported a single normal bowel motion at commencement of symptoms with no further flatus or bowel motions. She had a history of asthma, hypertension and a previous appendicectomy. On examination, she had a soft, but distended abdomen with mild generalized tenderness without features of peritonitis. A computed tomography (CT) scan of the abdomen and pelvis identified a colonic intussusception affecting the transverse colon and an ~6-cm colonic lipoma that likely reflected the lead point causing large bowel obstruction (Fig. 1). An emergency laparotomy identified a large lipomatous mass at lead point with a transverse colon intussusceptum into descending colon intussuscipiens (Fig. 2). Gentle traction reduced the intussusception, and no bowel compromise was identified. The mass was situated proximal to the middle colic vessels. Given the colonic location and due to the risk of malignancy, a right hemicolectomy was performed with high ligation and division of the ileocolic vessels. An ileocolic anastomosis was constructed using a stapled side-to-side functional end-to-end technique. The patient had an uncomplicated post-operative recovery and was discharged on day six. Histopathology confirmed the presence of two lipomas: the first being a large pedunculated mass within the distal aspect of the resection and the second arising within the ileocecal valve. No atypical features were identified (Fig. 3).

Contrast-enhanced CT of the abdomen demonstrating large bowel intussusception involving the transverse colon (arrow).
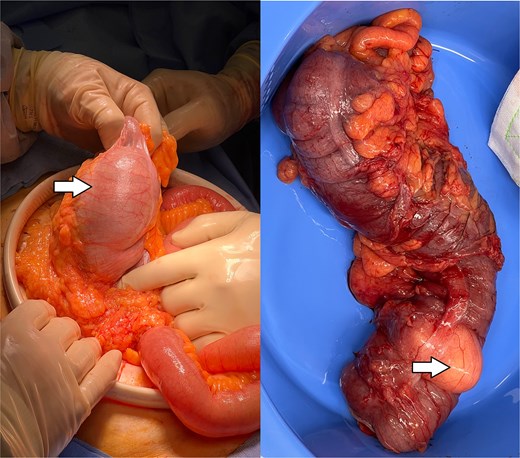
Intraoperative findings. Left: Reduced intussusception with visible intraluminal lead point (arrow). Right: Resected bowel demonstrating lipoma (arrow).
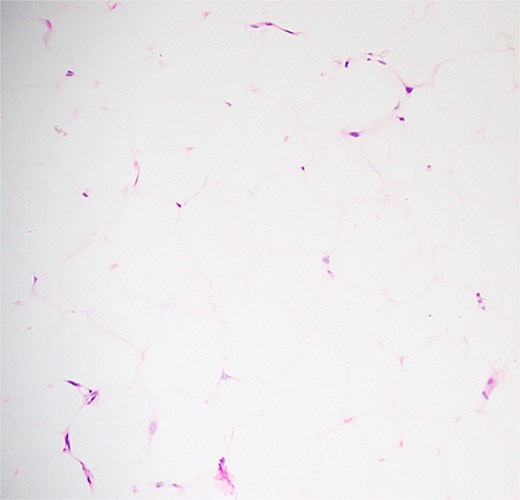
Histopathology showing benign adipose tissue without atypia, lipoblasts, necrosis, or mitotic activity.
Discussion
Adult intussusception accounts for ˂5% of all cases [1]. Due to its low prevalence and non-specific symptoms, intussusception is often only diagnosed on imaging or intra-operatively [4]. CT is the most sensitive imaging modality but cannot always distinguish benign from malignant lead points [5]. Features suggesting malignancy include irregular margins, wall thickening, and lymphadenopathy [6]. A lipoma appears as a well-circumscribed, ovoid, homogeneous fat-attenuation lesion [7]. In our patient, CT demonstrated these classic lipoma features; however, due to the colonic location and the risk of malignancy, we proceeded with en-bloc resection without reduction.
The differential diagnosis of a colonic lead point includes not only lipoma but also adenomatous polyps, complicated diverticulosis, neurofibroma, haemangioma, leiomyoma, and pseudolipomatosis [8]. Well-differentiated liposarcoma must be excluded, as stromal atypia may be present microscopically [9].
Intussusception is primary (no lead point) or secondary (pathological lead point). Secondary cases constitute the majority in adults [2, 10]. Pathological lesions include malignant and benign tumours; the likelihood of either one causing intussusception depends on the segment of bowel affected. In adults, small bowel intussusception is more likely to be caused by a benign lesion [5]. In colonic cases, including ileo-caecal, ileo-colic, and colo-colic intussusception, malignant tumours are more frequent [5, 10]. A 2025 systematic review of 2330 adult patients reported malignancy in 68% of colocolic intussusceptions, compared with only 9% of small bowel cases [2]. This evidence strongly supports en-bloc oncological resection without attempted reduction in colonic intussusception. Colonic lipoma causing intussusception is uncommon. A 2021 review of 117 lipoma-induced intussusception cases (mean size 5.1 cm, mean age 54.5 years) reported no malignancy at the lead point [7]. Our case aligns with this profile.
The pathophysiological mechanism involves the lipoma acting as a lead point, propelled distally by peristalsis [7]. Factors increasing intra-abdominal pressure, such as chronic constipation or straining, may precipitate telescoping [11]. Redundant colon may also predispose to intussusception [12].
Most colonic lipomas (90%) are submucosal, as in our case; less commonly subserosal or intramuscular [6, 7]. Submucosal lipomas are prone to pedunculation and intussusception [7]. Most authors recommend emergency colon resection, though opinions vary on bowel manipulation and resection extent. Some argue that manipulation risks tumour seeding, so all colonic intussusceptions should be resected en-bloc without reduction due to the high likelihood of underlying malignancy [5]. On the contrary, others propose that if a benign lesion is strongly suspected pre-operatively or via intraoperative colonoscopy, it may be appropriate to perform manual reduction before resection to minimize the length of bowel resected [13]. Resection of benign lesions can be performed both endoscopically and surgically. Endoscopic techniques include endoscopic mucosal resection, endoscopic submucosal resection, and dissection with loop-assisted snare or ligation [7, 13]. Surgical intervention involves the removal of the affected bowel segment and may vary from a segmental colectomy to a more extensive formal resection, such as an extended right colectomy, with options for either laparoscopic or open approaches. Surgical resection is recommended when benign lesions are complicated by intussusception, as in this case [7]. In general, most authors suggest a surgical approach aligned with appropriate oncological resection, including resection of the lead point, and then anastomosis between healthy and viable tissue [13]. If there is any suspicion for malignancy, reduction should not be attempted due to the risks of tumour seeding and dissemination. Similarly, reduction should be avoided if there is evidence of bowel ischemia due to the risks of perforation and subsequent abdominal contamination. Additionally, in cases of significantly co-morbid patients with evidence of bowel inflammation or oedema, the consideration of stoma formation versus primary anastomosis may be appropriate [5]. The management approach should be individualized to each patient, considering factors such as the lesion’s location, size, pathology, and associated complications.
An incidental finding was a second synchronous lipoma at the ileocaecal valve. Synchronous colonic lipomas are rarely reported [14]. This suggests that intraoperative palpation of the entire colon may be prudent when one lipoma is identified.
This case highlights that colonic intussusception, though rare, can result from benign lesions like lipomas. Pre-surgical imaging aids in identifying lead point characteristics. Management should be tailored to the individual patient, balancing clinical presentation with suspected pathology.
Conflicts of interest
The authors declare no conflicts of interest.
Funding
The authors declare that no funding was received.
Consent to participate and consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.

{kind=link}
{kind=link}
{kind=link}