





Abstract
Accurate intraoperative identification of parathyroid glands is essential to prevent hypoparathyroidism after thyroidectomy. Near-infrared autofluorescence is an emerging adjunct, and the PTeye system enables real-time, label-free detection of parathyroid tissue. We report an initial case series of three patients undergoing total thyroidectomy, with or without central lymphadenectomy, in a spoke center. PTeye was used intraoperatively to assist parathyroid identification. Three patients (68M, 57F, 49F) underwent surgery, with operative times of 88, 66, and 73 min. In all cases, PTeye enabled identification of four parathyroid glands without interfering with neuromonitoring. No inadvertent parathyroidectomy was observed. Postoperative calcium and parathyroid hormone levels remained within normal ranges. PTeye appears to be a feasible and safe adjunct for parathyroid identification during thyroidectomy. Further studies are required to confirm its impact on clinical outcomes.
Introduction
Postoperative hypoparathyroidism remains one of the most frequent complications following thyroid surgery, with transient hypocalcemia reported in up to 30% of cases [1, 2]. Accurate identification and preservation of the parathyroid glands are essential to reduce this risk.
Intraoperative identification traditionally relies on visual assessment, which may be challenging in cases of distorted anatomy, inflammatory disease, or central lymphadenectomy. Near-infrared autofluorescence (NIRAF) has emerged as a promising technique for real-time identification of parathyroid tissue without exogenous contrast agents [3, 4].
The PTeye system is a handheld probe that detects intrinsic parathyroid autofluorescence, providing immediate feedback through direct tissue contact [5, 6].
Most available evidence derives from high-volume centers, while data from lower-volume or spoke centers remain limited.
We report our initial case series describing the use of PTeye during thyroidectomy in a spoke center.
Case series
We describe three consecutive patients who underwent thyroidectomy with intraoperative PTeye-assisted parathyroid identification between January and March 2025 at our institution. Indications for surgery were based on cytological or clinical findings. None had preoperative hypocalcemia or known parathyroid disease.
Patient characteristics and surgical data are summarized in Table 1.
Patient characteristics and surgical data
| Patient | Age | Sex | Diagnosis | Procedure | Operative time | Parathyroids identified |
|---|---|---|---|---|---|---|
| 1 | 68 | M | Medullary thyroid carcinoma | TT + CCLND | 88 min | 4 |
| 2 | 57 | F | Multinodular goiter | TT | 66 min | 4 |
| 3 | 49 | F | Thyroid nodule TIR 3B | TT | 73 min | 4 |
All patients underwent preoperative biochemical evaluation including serum calcium, parathyroid hormone (PTH), and thyroid function tests. Flexible laryngoscopy was performed preoperatively and postoperatively to assess vocal cord mobility. Chest radiography was obtained preoperatively to evaluate tracheal anatomy.
Postoperative biochemical monitoring included serum calcium and PTH measurements at postoperative Day 1. Follow-up biochemical assessment, including calcium, PTH, and thyroid-stimulating hormone, was performed 30 days after surgery.
The institutional reference ranges were 8.5–10.5 mg/dl for serum calcium and 15–65 pg/ml for PTH.
All procedures were performed by the same surgical team using intermittent intraoperative neuromonitoring.
The PTeye system was used after exposure of suspected parathyroid tissue, providing real-time visual and auditory confirmation of autofluorescence.
The intraoperative workflow consisted of visual identification of suspected parathyroid tissue followed by direct probe contact to confirm autofluorescence before further dissection. This stepwise approach allowed rapid confirmation without interrupting the surgical procedure (Fig. 1).
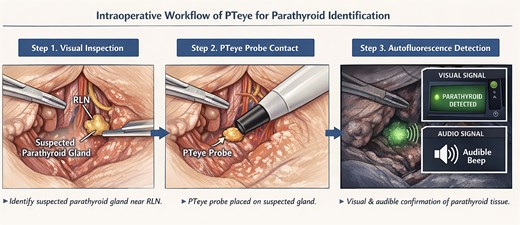
Schematic illustration of the intraoperative workflow for PTeye-assisted parathyroid identification.
The device was used according to the following intraoperative steps:
Surgical exposure of the thyroid lobe and identification of the main anatomical landmarks, including the recurrent laryngeal nerve and the superior and inferior thyroid poles.
Visual identification of tissues suspected to represent parathyroid glands based on their typical anatomical location and macroscopic appearance.
Direct contact of the PTeye probe with the suspected tissue before further surgical manipulation (Fig. 2a).
Real-time confirmation of parathyroid autofluorescence through the device’s visual and auditory feedback system (Fig. 2b).
Preservation of the identified parathyroid gland and continuation of surgical dissection.
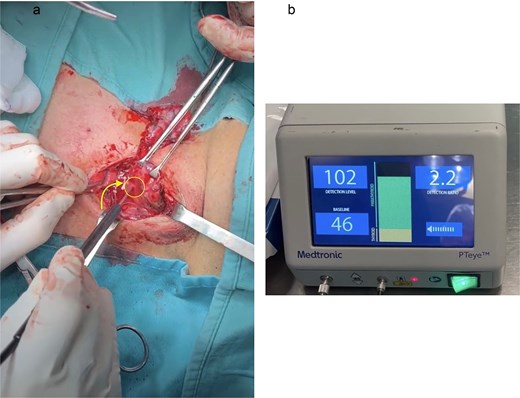
Intraoperative identification of a parathyroid gland using the PTeye autofluorescence probe. (a) Intraoperative view during thyroidectomy showing a suspected parathyroid gland (arrow) located beneath the PTeye probe. (b) PTeye console display demonstrating detection of parathyroid tissue with a characteristic autofluorescence signal.
This workflow allowed rapid confirmation of parathyroid tissue without interrupting the surgical procedure or modifying the standard operative steps.
Operative and biochemical findings are summarized in Tables 1 and 2.
Perioperative calcium and PTH levels
| Patient | Pre-op Ca | Pre-op PTH | Ca POD1 | PTH POD1 |
|---|---|---|---|---|
| 1 | 9.4 | 34 | 8.9 | 28 |
| 2 | 10.0 | 38 | 8.9 | 33 |
| 3 | 8.7 | 43.2 | 9.1 | 39.4 |
Three patients underwent thyroidectomy using PTeye. Operative times were 88, 66, and 73 min, comparable to standard procedures at our institution.
In all cases, four parathyroid glands were identified intraoperatively using the PTeye probe. The device facilitated differentiation between parathyroid tissue and surrounding structures.
No intraoperative complications occurred. Histopathological examination confirmed the absence of inadvertent parathyroidectomy.
Postoperative serum calcium and PTH levels were within normal ranges at postoperative Day 1 in all patients. At 30-day follow-up, biochemical values remained normal, with no cases of hypocalcemia.
This work has been reported in accordance with the SCARE criteria.
Discussion
Accurate intraoperative identification of parathyroid glands is critical for preventing postoperative hypocalcemia. Despite surgical experience, identification may be challenging in complex anatomical settings.
NIRAF has emerged as a useful adjunct for real-time identification of parathyroid tissue. Previous studies have shown that parathyroid glands emit a characteristic autofluorescence signal, allowing differentiation from surrounding tissues and improving intraoperative recognition compared with visual inspection alone [3, 5, 6, 7].
The PTeye system provides point-of-contact confirmation through a probe-based approach, without requiring additional imaging systems. In our experience, it functioned as a confirmatory tool supporting intraoperative decision-making rather than replacing surgical judgment.
In this series, PTeye enabled identification and preservation of all parathyroid glands without increasing operative time or interfering with neuromonitoring. Integration into the surgical workflow was straightforward and did not require modification of standard techniques.
Notably, the learning curve associated with the device appeared minimal, and integration into routine thyroid surgery was rapid even in a spoke-center setting.
This experience reflects a spoke-center environment, where adjunctive technologies may support standardization of surgical performance and enhance intraoperative safety.
Postoperative biochemical outcomes were favorable, with no cases of hypocalcemia. Although causality cannot be established due to the small sample size, these findings are consistent with improved intraoperative identification.
The present report is limited by the descriptive nature of the series, the absence of a control group, and the small number of patients. Larger studies are needed to evaluate the clinical impact of probe-based autofluorescence technologies.
Conclusion
The PTeye system is a feasible and easily implementable adjunct for intraoperative parathyroid identification during thyroidectomy. It allows reliable recognition of parathyroid tissue without interfering with surgical workflow or operative time.
In this preliminary experience, all parathyroid glands were preserved, with no cases of hypocalcemia or inadvertent parathyroidectomy.
Probe-based autofluorescence may represent a practical tool to support intraoperative decision-making, particularly in lower-volume centers. Further studies are required to confirm its impact on postoperative outcomes.
Author contributions
E.C.: Study design, Surgery, Manuscript preparation; C.G.: Manuscript revision; D.G.: Data collection, Manuscript review; R.P.: Surgical procedures; G.B.: Perioperative management; L.S.: Surgical assistance; O.Z.E.: Data collection; Y.P.V.: Surgical assistance; V.T.: Scientific supervision; M.S.: Manuscript revision; M.G.: Manuscript revision; A.F.: Manuscript revision; and M.T.: Study supervision. All authors contributed to the study conception, data collection, analysis, and manuscript preparation. All authors read and approved the final manuscript.
Conflicts of interest
The authors declare that they have no competing interests.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Data availability
The datasets generated and analyzed during the current study are not publicly available due to privacy considerations but are available from the corresponding author upon reasonable request.
Ethics approval and consent to participate
All procedures performed in this study involving human participants were conducted in accordance with the ethical standards of the institutional research committee and with the 1964 Declaration of Helsinki and its later amendments.
The study was approved by the Institutional Review Board / Ethics Committee of the G. Paolo II Hospital (Azienda Sanitaria Provinciale, Lamezia Terme, Italy).
All patients provided written informed consent for treatment and for the use of anonymized clinical data for research and publication purposes.
Consent for publication
Written informed consent was obtained from all patients for publication of anonymized clinical data and images.

{kind=link}
{kind=link}