





Abstract
Mucinous cystic neoplasms (MCNs) of the pancreas are slow-growing tumours but carry a risk of malignant transformation and massive enlargement if left untreated. We present a rare case of a 49-year-old female initially diagnosed in 2022 with a 14-cm pancreatic cyst. After declining surgery, she presented four years later with acute bowel obstruction and a distended abdomen. Imaging revealed dramatic progression to a giant 31 × 22.7 cm mass displacing most abdominal viscera. An emergency distal pancreatectomy and splenectomy were performed, followed by a staged second-look laparotomy to ensure colonic viability. Despite the massive size, tumour markers remained normal. Histopathology confirmed MCN with focal high-grade dysplasia but no invasive carcinoma. This case demonstrates that extreme mass effect from a giant MCN can cause acute intestinal obstruction and emphasizes that size alone, while increasing surgical complexity, is not an absolute predictor of invasive malignancy.
Introduction
Mucinous cystic neoplasms (MCNs) are distinct pancreatic cystic tumours characterized by a pathognomonic ovarian-type stroma and a nearly exclusive occurrence in females. Typically located in the body or tail of the pancreas, these lesions are recognized for their potential to transform into invasive adenocarcinoma [1]. Consequently, international consensus guidelines, including the Fukuoka 2017 criteria, advocate for surgical resection in fit patients to prevent the risk of malignancy [2].
While MCNs are well-documented, ‘giant’ variantsspecifically those exceeding the 30 cm mark remain exceedingly rare in the surgical literature [3–5]. These cases present significant technical challenges during surgery due to the massive displacement of surrounding organs and the risk of acute mechanical complications [5, 6]. We report this 31 cm case to document the progression of an MCN over a 4-year period and to discuss the surgical management of markedly large pancreatic lesions recorded to date.
Case report
A 49-year-old female with a medical history of a prior stroke and uterine fibroids was initially evaluated in 2022 for vague abdominal discomfort. A contrast-enhanced computed tomography (CT) at that time identified a 14 × 14.5 × 16 cm cystic lesion in the pancreatic tail, highly suggestive of an MCN (Fig. 1). Despite clinical counseling regarding the risks of growth and malignancy, the patient refused surgical intervention and missed her scheduled follow-up appointments.
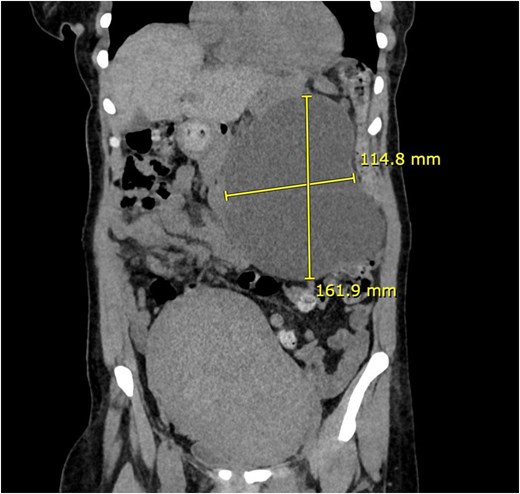
Baseline CT (2022). Coronal CT abdomen (2022) showing 16.1 × 11.4 cm pancreatic cystic lesion. Notably, a large co-existing uterine fibroid is seen in the pelvis.
Over the following four years, she suffered from chronic abdominal pain and developed progressive obstructive symptoms. This was a gradual process, beginning with an inability to tolerate solid food, which eventually progressed by early 2026 to a complete inability to tolerate any oral intake. The patient presented to emergency department with abdominal pain, vomiting, and obstipation, with a distended abdomen consistent with complete bowel obstruction. Upon admission, nasogastric tube was inserted achieving significant decompression.
Imaging revealed the mass had grown to 31 × 22.7 × 24 cm, displacing most abdominal viscera (Fig. 2). The small bowel loops were severely compressed by the mass without a clear transition zone, suggesting a mechanical obstruction caused by direct mass effect and displacement of the intestinal loops.
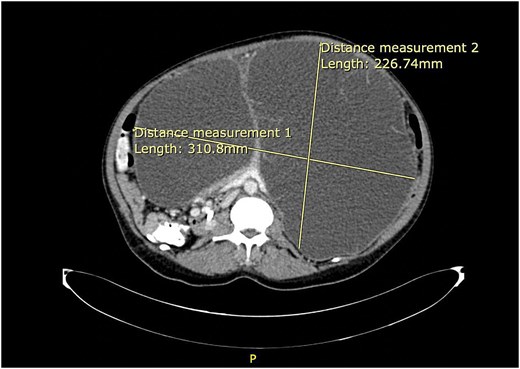
Preoperative progression (2026). Preoperative axial contrast-enhanced CT demonstrating a massive pancreatic mucinous cystic neoplasm (MCN) (31.08 × 22.67 cm). The mass occupies the entire abdominal cavity, causing complete visceral displacement and posterior compression of the retroperitoneal great vessels.
Investigations
Laboratory tests showed anaemia; however, serum amylase, liver function, and kidney function were within normal ranges. Notably, tumour markers were not elevated: CA 19-9 was <37 U/ml and carcinoembryonic antigen test (CEA) was <5 ng/ml. A repeat contrast-enhanced CT demonstrated a multiloculated cystic mass, replacing the pancreatic body and tail, showing peripheral calcifications and significant mass effect that displaced the stomach and compressed the colon (Fig. 3).
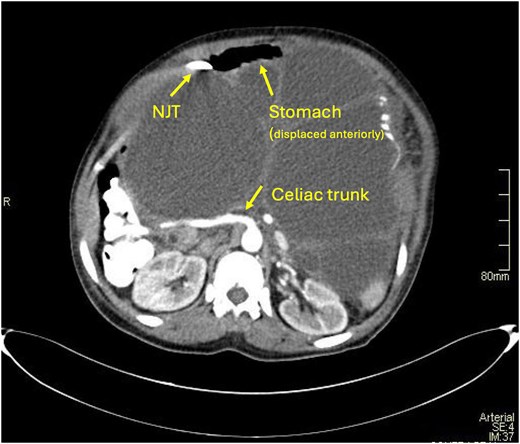
Axial CT image highlighting the significant mass effect. The giant MCN causes extreme anterior displacement and compression of the stomach (with NJ tube in situ). Additionally, it demonstrates the posterior displacement of the celiac trunk.
Detailed vascular mapping showed significant superior displacement and stretching of the celiac axis, specifically involving the common hepatic and left gastric arteries (Fig. 4).
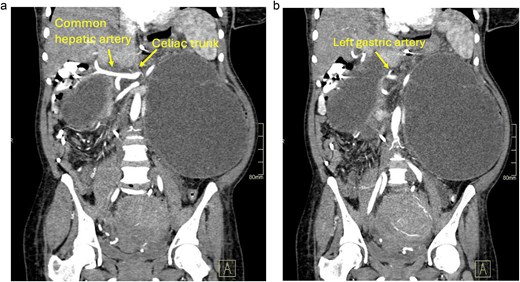
Vascular mapping coronal CT image highlighting the critical vascular relationship. The giant MCN exerts a severe mass effect on the celiac axis, causing significant superior displacement and stretching of the left gastric artery, and the common hepatic artery.
Surgical management
Given the acute obstructive symptoms, the patient was taken for emergency exploratory laparotomy. Long midline laparotomy was performed. Upon exploration, a giant cyst was found with extensive adhesions to surrounding structures, specifically the splenic hilum and the transverse mesocolon (Figs 5 and 6).
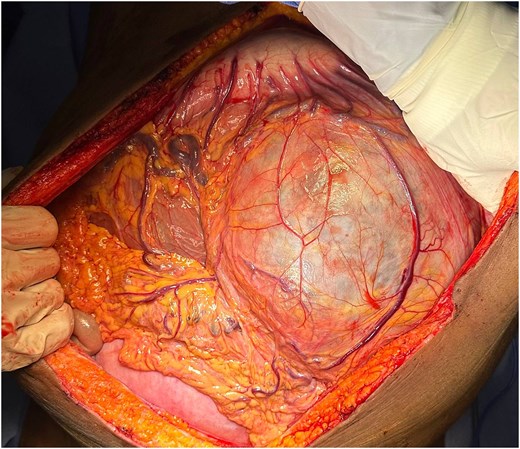
Intraoperative view following exploratory laparotomy. A giant, well-encapsulated multiloculated cystic mass is seen occupying almost the entire abdominal cavity, causing significant displacement of the omentum and surrounding viscera.
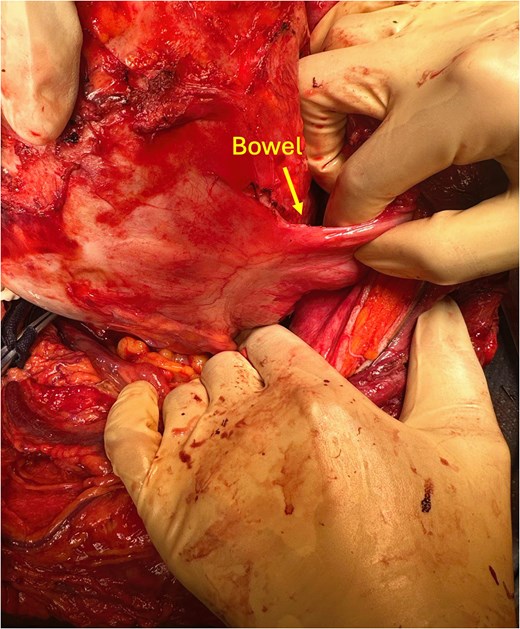
Intraoperative image demonstrating dense adhesions between the giant cystic mass and the adjacent bowel loops (marked).
Meticulous adhesolysis and a distal pancreatectomy and splenectomy were performed with care to maintain cyst integrity (Fig. 7). Vascular control was meticulously achieved through combination of suture ligation and application of hemoclips and splenic vessel were managed with ligation. For the pancreatic transection, the pancreatic neck was divided using gastrointestinal anastomosis (GIA) linear stabler. The total estimated blood loss 300 ml with an operative time of 8 hours.
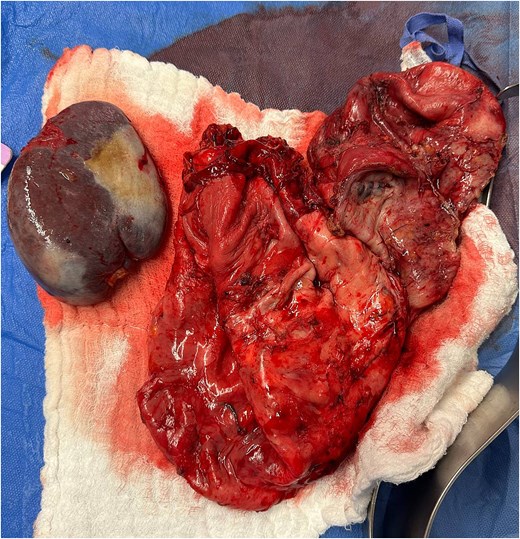
Final specimen. Gross surgical specimen showing the 31-cm multiloculated pancreatic cyst resected with the spleen.
Due to concerns regarding the viability of the chronically displaced descending colon, a staged approach with a programmed second-look laparotomy was adopted. The abdomen was temporarily closed using Bogota bag, and re-exploration 24 hours later confirmed bowel viability, allowing for definitive closure.
Postoperative outcome
The patient’s recovery was uneventful. Drain fluid amylase on post-operation day (POD) 3 was 14 U/L, ruling out a pancreatic fistula. She was discharged on POD 7. Following splenectomy patient received post-operative preventive care including administration of vaccination against encapsulated organisms. Furthermore, the patient and her family were counselled regarding the lifelong risk of overwhelming post-splenectomy infection. Histopathological examination confirmed a MCN. Grossly, the specimen measured 30 × 20 cm, and the pancreatic tissue was noted to be significantly obliterated by the massive multilocular cyst. Microscopically, the cyst was lined by mucin-secreting epithelium showing focal moderate to high-grade dysplasia. The underlying cyst wall demonstrated cellular ovarian-type stroma, confirmed by positive immunohistochemical staining (PR, Inhibin, and CD10). Invasive carcinoma was meticulously excluded through extensive sampling, with no evidence of stromal invasion. The surgical margins were clear, and the resected spleen showed only congestion. Although the initial 6-week follow-up showed excellent recovery with no early complications, a long-term surveillance plan has been established. This includes physical examination and CT imaging every 6 months for the first 2 years, followed by annual reviews to monitor for any late recurrence or potential malignant progression, given the high-grade dysplasia found in the pathology.
Discussion
The clinical course of this patient spanning 4 years of documented progression from a 14 cm lesion to a 31 cm mass provides a rare opportunity to observe the clinical evolution of an MCN in the absence of timely surgical intervention. In our patient, the lesion exhibited a calculated growth rate of ~4.2 cm per year, which is significantly higher than the average growth rates typically reported for MCNs [7]. This rapid expansion aligns with other rare reports of giant MCNs that showed accelerated growth over a short period, such as the case documented by Carvalho et al. [8].
A primary focus of this case is the Size-Malignancy Paradox. According to the Fukuoka international consensus guidelines, a cyst diameter of 3 cm or greater is established as a significant ‘worrisome feature’ in pancreatic cystic neoplasms, necessitating strong consideration for surgical resection [2]. Our patient presented with a mass measuring 31 cm, representing more than ten times the clinical threshold established for intervention. Despite this extreme dimension, the final pathology revealed focal high-grade dysplasia with no evidence of stromal invasion [9, 10]. This confirms that while massive size significantly increases surgical complexity, it does not serve as a definitive indicator of invasive adenocarcinoma. Furthermore, the fact that tumour markers (CEA and CA 19-9) remained within normal ranges despite the high-grade dysplasia highlights that normal serology can be deceptive and should not delay intervention for a rapidly growing pancreatic cyst [11, 12].
The surgical management was particularly challenging due to the distorted anatomy and the ‘obliterated pancreas’ in the body and tail. There were dense adhesions to the splenic hilum, bowel and the transverse mesocolon, requiring meticulous adhesolysis to ensure the cyst remained intact and to avoid intraoperative rupture [5, 6]. Given the massive size and chronic displacement of the bowel, the programmed second-look laparotomy was essential to ensure the viability of the descending colon and assess for delayed ischemic changes before final closure [13, 14].
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}