





Abstract
Secondary aortoenteric fistula is a rare and life-threatening complication following aortic reconstructive surgery, most commonly involving the duodenum. Erosion of an aortofemoral bypass graft into the sigmoid colon is exceptionally uncommon; all reported cases were managed via open surgery with significant morbidity. Laparoscopic management with graft preservation has not been documented. A 59-year-old man presented with massive hematochezia 9 months after bilateral aortobifemoral bypass for an abdominal aortic and common iliac aneurysm. Colonoscopy revealed a vascular graft 25 cm from the anal verge. Computed tomography confirmed penetration of the graft into the sigmoid lumen without abscess or contrast extravasation. The patient underwent laparoscopic sigmoid colectomy with graft preservation and peritoneal coverage, followed by colorectal anastomosis and defunctioning ileostomy. He was discharged on postoperative Day 7. He was maintained on a 6-week course of targeted oral antimicrobial therapy. At 6-month follow-up, the patient remains well with a patent graft, no recurrent bleeding, and no graft-related complications. This case highlights the feasibility of minimally invasive management and selective graft preservation in carefully selected patients, challenging the paradigm of mandatory graft excision.
Introduction
Late complications of aorto-femoral grafts include graft thrombosis, graft pseudoaneurysms, hernias, graft infections, and aortoenteric fistulas or graft migration. Aortoenteric fistula is a rare but potentially fatal complication following aortic reconstructive surgery with an annual incidence of 0.36%–1.6%. Mortality is at least 30% in most cases [1, 2]. Typically, it occurs secondary to an erosion of the proximal suture line on the aorta through the third or fourth portion in the duodenum [3]; while involving the sigmoid colon is exceedingly rare, with few cases reported, it presents with lower gastrointestinal bleeding and/or signs of sepsis [4].
Graft infection and pressure necrosis have been implicated as a cause in this situation. Other causes may include trauma, foreign body perforation, penetrating ulcers, tumour invasion, and radiation therapy [5].
Management of aortofemoral graft erosion into the sigmoid colon typically involves sigmoid colectomy, usually by open surgical approach, and to the best of current knowledge, no prior laparoscopic approach has been reported.
Case Report
A 59-year-old man subjected to bilateral aortobifemoral bypass graft surgery for an abdominal aortic and common iliac aneurysm. Nine months after surgery, he was presented with a severe attack of bleeding per rectum (~1000 cc). Clinically, the patient was hemodynamically unstable, appeared pale, heart rate was 125 beats/min, blood pressure was 90/60 mm Hg, and haemoglobin level was 8.3 g/dl. The patient was immediately resuscitated: two large-bore IV lines were placed, crystalloids were infused, and the massive transfusion protocol was activated to deliver Packed rec blood cells (PRBCs), plasma, and platelets (1:1:1). The patient was investigated by colonoscopy, which revealed a whitish tubular foreign body (vascular graft) 25 cm from the anal verge (Fig. 1). A contrasted computed tomography (CT) scan of the abdomen and pelvis revealed that the left-side aortofemoral graft kinked at its middle segment, which was visualized traversing the lumen of the sigmoid colon, yet there was no contrast extravasation and no extraluminal abnormal fluid collection (Fig. 2).

Endoscopic image of the colon showing a pale tubular vascular graft protruding within the colonic lumen, adjacent to the surrounding mucosal wall.
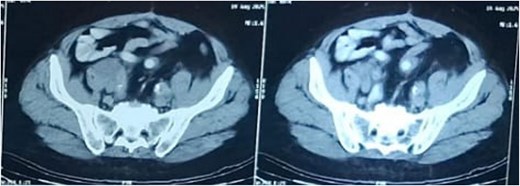
Axial contrast-enhanced CT scans of the pelvis showing erosion of the left limb of the aortobifemoral graft into the sigmoid colon.
The patient was prepared for laparoscopic sigmoid colectomy with preservation of the graft. Correction of anaemia with blood transfusion was done. Given the transient colonic contamination of the graft surface, perioperative broad-spectrum intravenous antibiotics were administered [piperacillin-tazobactam for 48 hours intraoperatively and during the intensive care unit (ICU) stay], followed by a 6-week course of oral targeted antimicrobial therapy. The decision to preserve the graft was based on the absence of perianastomotic fluid, abscess, or radiological features of graft infection on preoperative CT, and was confirmed intraoperatively by the absence of purulence, friable tissue, or gross contamination around the graft limb. A postoperative surveillance plan was established, including clinical assessment and CT angiography at 3 months to evaluate graft patency and exclude delayed perigraft sepsis.
Surgical technique
The patient was placed in the lithotomy position. A 10-mm port was placed above the umbilicus, a 5 mm right upper quadrant port, a 5 mm left side port, and a 12 mm right lower quadrant port. Insufflation was started by a Veress needle inserted at Palmer’s point; a 10 mm Visiport trocar was first inserted above the umbilicus. We mobilized the sigmoid colon through the medial to lateral approach, and we identified the right ureter, the sacral promontory, and the inferior mesenteric artery (IMA) pedicle. Once the pedicle is placed on a gentle traction, a mesenteric window was created. The pedicle was lifted upwards, and a gentle dissection was made in the proper congenital fusion plane between the mesentery and retroperitoneum. Once the mesentery was lifted off the retroperitoneum. A high ligation of the IMA, as it allowed visualization of the tissue planes. The colon was grasped and retracted medially. The colon was mobilized off the retroperitoneum by dissecting through the thin lateral peritoneal layer. The proximal end of the sigmoid colon was transected with a laparoscopic linear cutter stapler, then the sigmoid was opened and removed from the migrating graft, which was preserved. Then the rectum was transected with a laparoscopic linear cutter stapler, ideally in one single firing. The graft is then covered by peritoneum to prevent future erosion. End-to-end colo-rectal anastomosis was done by using a trans-anal circular stapler. Covering defunctioning ileostomy also was done (Fig. 3F).
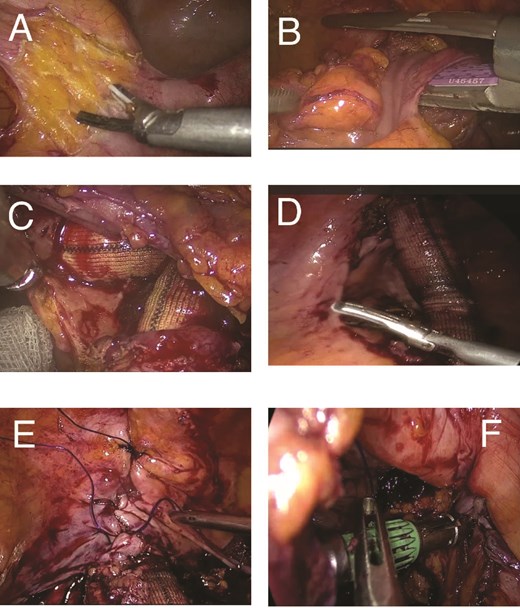
Laparoscopic approach for sigmoid colectomy. (A) Creation of the mesenteric window using an ultrasonic energy device. (B) Transecting proximal end of the sigmoid colon with the linear stapler. (C) The graft emerging into the colon. (D) Freeing the sigmoid colon from the graft. (E) Covering the graft by peritoneum. (F) Creating the Colo-rectal anastomosis by the trans-anal circular stapler.
Postoperatively, the patient was admitted to the intermediate surgical ICU for 2 days, then started oral fluid and soft food; one week later, the patient was discharged from the hospital. At the 3-month outpatient visit, CT angiography demonstrated a patent aortobifemoral graft with no perigraft fluid collection, perianastomotic abscess, or radiological features of graft infection. No biochemical or clinical signs of sepsis were observed during the follow-up period. The defunctioning ileostomy was reversed at 12 weeks postoperatively without complication. At 6-month follow-up, the patient remains clinically well, with no recurrence of gastrointestinal bleeding, no anastomotic failure, and no evidence of re-erosion or graft-related sepsis on surveillance imaging.
Discussion
Aortoenteric fistula (AEF) can be classified into primary and secondary. Primary AEF forms spontaneously in the absence of a synthetic aortic graft. This is a rare cause (<1:1000) of gastrointestinal (GI) bleeding. Most primary fistulas are due to malignancy arising in the GI tract [6, 7].
Secondary AEFs are fistulas that develop in the presence of a synthetic aortic graft and were first described by Brock in 1953 [8]. Secondary AEF usually occurs years after aortic reconstructive surgery, although it can present anytime from 6 months to > 10 years postoperatively [9]. It may be associated with chronic infection around the graft, bleeding per rectum, abdominal pain, retroperitoneal abscesses, and back pain [9]. Secondary AEF needs urgent surgical intervention. The survival rate without intervention is poor [2]. A few cases of sigmoid perforation by aortofemoral graft were reported in the literature; a review of published cases of sigmoid colon erosion by aortofemoral grafts demonstrates that all reported patients were managed via open surgery, often involving graft excision, bowel resection, and extra-anatomic bypass. While effective, these approaches are associated with substantial operative trauma, prolonged recovery, and high perioperative risk, particularly in haemodynamically unstable patients. Table 1 shows recent reported similar cases. In contrast, in the present case a minimally invasive laparoscopic approach was selected, particularly in the absence of graft infection, abscess formation, or uncontrolled hemorrhage. Preservation of the vascular graft was possible due to the lack of radiologic or intraoperative evidence of infection, allowing avoidance of complex vascular reconstruction. This approach offers several potential advantages, including reduced surgical trauma, improved visualization of pelvic structures, faster postoperative recovery, and preservation of vascular continuity. Importantly, complete peritoneal coverage of the exposed graft was performed to minimize the risk of recurrent erosion. From a surgical perspective, this case expands the available surgical options and suggests that laparoscopy may be considered a valid alternative to open surgery in selected patients, provided that meticulous preoperative imaging and multidisciplinary planning are undertaken.
Summary of published case reports describing secondary aortoenteric fistula involving the colon.
| Author/ Year | Age/Sex | Presentation | Previous surgery (timing) | Etiology | Site of erosion | Surgical approach | Graft management | Outcome | Notes |
|---|---|---|---|---|---|---|---|---|---|
| Current Case (2026) | 59 M | Hematochezia + shock | Bilateral aorto-bifem bypass (9mo) | Mechanical erosion (noninfected) | Sigmoid | Laparoscopic sigmoid resection + anastomosis | Preserved + peritoneal coverage | Uneventful, <30d follow-up | Possibly the first reported laparoscopic approach |
| Brock (1953) [7] | 44 F | GI bleeding | AAA homograft (3mo) | Suture line erosion | Duodenum | Open duodenal repair | Graft removed | Survived | First reported SAEF |
| Perez (2005) [10] | 62 M | Hematochezia | Aortobifemoral bypass | Mechanical erosion | Sigmoid | Open Hartmann + axillobifemoral bypass | Explant | Stable | Rare sigmoid SAEF |
| Wiangphoem (2022) [11] | 65 M | Hematochezia + pain | EVAR (6mo) | Infective erosion | Sigmoid | Staged open bypass → Hartmann | Explant | Good, 1mo discharge | Staged open repair |
| Goda (2019) [12] | 64 M | Atypical pain, anorexia | Open AAA (1 yr) | Mechanical | Duodenum | Open segmental resection | Preserved + omentum | 40-day stay, survived | Successful graft preservation |
| Abu Jheasha (2023) [13] | 63 M | Double bleeding + sepsis | Juxtarenal AAA + bypass | Graft infection | Duodenum + Cecum | Two-stage open | Explant | Discharged stable | Double SAEF (rare) |
| Chaulagain (2025) [14] | 36 M | Melena, shock | Aorto-CFA + CIA bypass (7 yr) | Infection | Duodenum | Open graft removal + bypass | Explant | Good | Nepal first case |
| Nakajima (2025) [15] | 71 M | Lower GI bleed + sepsis | Open AAA (4mo) | Infection | Sigmoid | Staged open → EVAR salvage | Replaced → stent | 5 yr stable | Hybrid salvage success |
AAA = Abdominal aortic aneurysm, AEF = Aortoenteric fistula, CIA = Common iliac artery, CFA = Common femoral artery, EVAR = Endovascular aneurysm repair
Conclusion
This case represents the first reported laparoscopic management of sigmoid involvement in secondary AEF with successful graft preservation. Erosion of aorto-femoral graft into sigmoid colon should be considered as one of the causes of GI bleeding in any patient with a history of aortic graft surgery. The treatment is urgent surgical intervention. A laparoscopic approach may represent a feasible management option with favorable short-term outcomes in carefully selected patients.
Author contributions
S.G. and M.A.A.M. performed the surgery and drafted the first manuscript. M.E.S. drafted and edited the manuscript. M.E.K. reviewed the literature. All authors read and approved the final manuscript.
Conflicts of interest
The authors declare that they have no competing interests.
Funding
No source of funding for this study.
Data availability
The data supporting the findings of this case report are available from the corresponding author upon reasonable request.
Ethical approval and consent to participate
Ethical approval was obtained from the Institutional Review Board of Al Azhar Faculty of Medicine, Cairo, Egypt.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
References
Rüütmann AM, Kals J. Primary and secondary aortoenteric fistulas in a patient with abdominal aortic aneurysm.
Cvjetko I.
Nakajima T, Shibata T, Miura S et al. A case of problem-free survival five years after abdominal aortic sigmoid colon fistula surgery. Cureus 2024;16:e75026.
Author notes
Sameh Gabr and Mohammed Arafat Abdel Maksoud contributed equally to this work.

{kind=link}
{kind=link}
{kind=link}