





Abstract
Dorsal chordee is a rare congenital penile curvature, typically diagnosed in childhood. Occult urethral anomalies in adults are uncommon and may remain undetected due to subtle presentation and incomplete medical history. We report a 22-year-old male presenting with dorsal penile curvature. Preoperative clinical evaluation and cystoscopy were normal. During corrective surgery, an incidental epispadiac urethral fistula was identified following leakage of lignocaine jelly after catheterization. A three-layer turn-over flap repair using preputial tissue was performed along with chordee correction. The postoperative course was uneventful, with excellent functional and cosmetic outcomes. The fistula was initially presumed congenital; however, operative findings and prior surgical history suggested a likely postoperative etiology following childhood distal epispadias repair. This case highlights the limitations of routine preoperative assessment and emphasizes the importance of intraoperative vigilance in detecting concealed urethral anomalies.
Introduction
Chordee refers to congenital penile curvature and is most commonly associated with ventral curvature and hypospadias. Isolated dorsal chordee without associated urethral anomalies is extremely rare and poorly documented in literature [1, 2]. While most cases are diagnosed and treated in childhood, delayed presentation in adulthood may occur.
Urethrocutaneous fistulas and epispadiac variants arise from abnormal urethral development. Minor defects may remain asymptomatic and undetected for years, particularly when urinary function is preserved [3]. The coexistence of dorsal chordee with an occult urethral fistula is exceptionally uncommon. We report a rare case in which a concealed epispadiac fistula was identified intraoperatively, underscoring the importance of surgical vigilance.
Case presentation
A 22-year-old male presented with dorsal penile curvature during erection since adolescence, causing cosmetic concern and mild discomfort. He reported a vague history of urethral surgery in infancy, with no available records. There were no urinary complaints, infections, trauma, or erectile dysfunction.
On examination, the penis was normally positioned with a retractable foreskin and a normal urethral meatus. Mild dorsal curvature was noted (Fig. 1a and b). No fistula or discharge was visible.
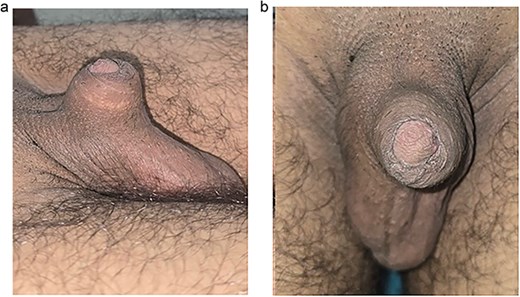
(a) Preoperative lateral view; (b) preoperative appearance – dorsal view. Preoperative photograph showing dorsal view of the penis with mild dorsal curvature and normal-appearing external meatus, with no obvious visible fistula. Lateral photograph demonstrating dorsal penile curvature consistent with dorsal chordee.
Investigations
Preoperative flexible cystoscopy revealed a normal urethra and bladder, with no evidence of strictures or fistulous communication. Routine laboratory investigations were unremarkable.
Surgical correction of dorsal chordee was planned under spinal anesthesia.
Surgical management
Following catheterization and foreskin retraction, leakage of lignocaine jelly was observed from the dorsal coronal region. Careful inspection revealed two small pin-point openings suggestive of urethrocutaneous communication (Fig. 2).
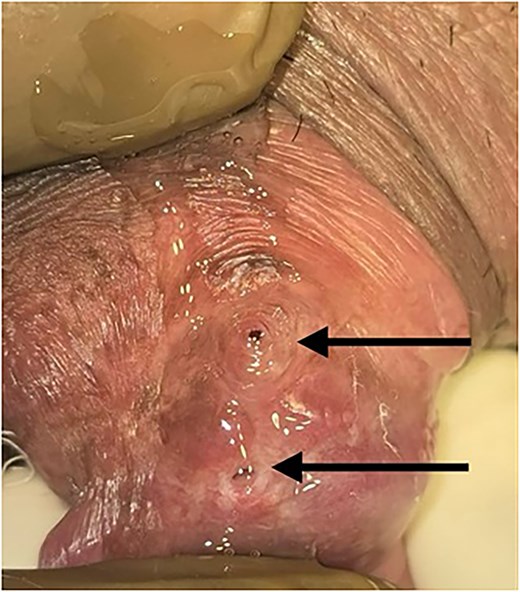
Dorsal coronal sulcus showing dual epispadiac openings. Magnified intraoperative view of the dorsal aspect of the coronal sulcus showing leakage of lignocaine jelly through two pin-point dorsal opening (indicated by arrows) following Foley catheter insertion confirming urethrocutaneous communication.
Two parallel incisions were made to expose and dissect the fistulous tract. The tract was excised and freshened. A three-layer repair was performed using a turn-over preputial flap: urethral mucosa closure, flap reinforcement, and tension-free skin closure (Fig. 3) Simultaneously, tunica albuginea scar tissue was released to correct dorsal curvature. A urethral catheter was retained for 10 days (Fig. 4).
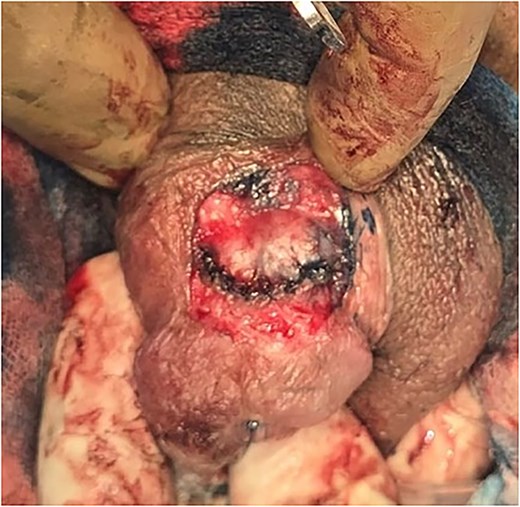
Intraoperative view of fistula repair site. Intraoperative image demonstrating exposed fistula tract after freshening of margins and preparation for layered closure.
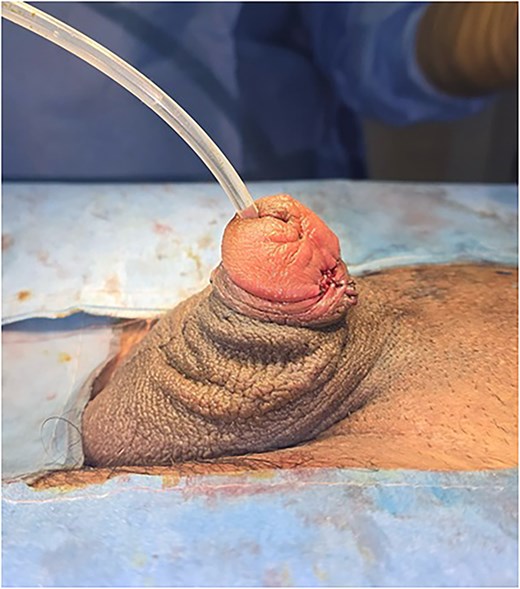
Postoperative appearance. Postoperative photograph showing satisfactory penile alignment and intact layered closure following urethral fistula repair and correction of dorsal chordee with silicon catheter draining clear urine.
The postoperative period was uneventful. After catheter removal, the patient demonstrated a good urinary stream with no leakage. At follow-up, satisfactory penile alignment and cosmetic appearance were achieved, with no recurrence.
Discussion
Isolated dorsal chordee without hypospadias is a rare congenital anomaly [1, 2]. Adult presentation is uncommon and may reflect delayed diagnosis or incomplete childhood treatment. The presence of an occult urethral fistula further adds to the rarity of this case.
Small urethral defects may remain undetected due to the absence of symptoms and normal urinary function [3]. In our patient, preoperative cystoscopy failed to identify the fistula, highlighting the limitation of endoscopic evaluation in detecting small external communications.
Previous studies have emphasized that small urethral fistulas may be missed unless meticulous inspection is performed [4, 5]. In this case, the fistula became evident only after catheterization, which resulted in leakage of lignocaine jelly. This underscores the importance of careful intraoperative assessment, particularly in patients with a history of prior urethral surgery.
Successful management of urethrocutaneous fistulas requires complete excision, tension-free closure, and multilayered reinforcement [6]. The three-layer turn-over flap technique provides well-vascularized coverage and reduces recurrence risk. In this case, it achieved excellent functional and cosmetic outcomes.
Simultaneous correction of chordee and fistula in a single-stage procedure can be effective in selected patients, provided adequate tissue quality and meticulous technique [5, 6].
In retrospect, considering the history of childhood penile surgery and the intraoperative findings, the fistulous tract was likely secondary to a prior distal epispadias repair, possibly a Thiersch-Duplay type urethroplasty, rather than representing a purely congenital occult lesion.
Conclusion
Dorsal chordee with an occult epispadiac urethral fistula is an exceptionally rare presentation in adulthood. Routine preoperative evaluation may fail to detect subtle anomalies. Intraoperative vigilance is essential for diagnosis, and multilayered repair techniques can achieve optimal outcomes.
Conflicts of interest
The authors declare no conflict of interest.
Funding
This study did not receive any funding.
Consent
Written informed consent obtained.

{kind=link}
{kind=link}
{kind=link}
{kind=link}