





Abstract
Syringocystadenocarcinoma papilliferum (SCACP) is a rare cutaneous adnexal neoplasm that may arise from head and neck subsites & often mimic other cystic lesions of neck. We report a case of a giant cystic neck swelling occupying the entire left half of neck posing diagnostic & therapeutic challenges. A nil comorbid man in his 90s presented with a progressive lateral neck swelling for 2 years. An Initial fine needle cytology was non-diagnostic. Magnetic resonance imaging demonstrated extensive involvement by the lesion across both the anterior and posterior triangles of the neck. The tumor was excised by transcervical approach. Final histology with cytokeratin 7,19 & SOX10 positivity suggested SCACP. This case highlights SCACP’s potential for massive, non-infiltrating growth in the neck, distinguishable from other cystic lesions through histology & immunohistochemistry. Successful transcervical excision in a geriatric patient, despite inherent challenges & low tumor aggressiveness reinforces the value of surgical management.
Introduction
Syringocystadenocarcinoma papilliferum (SCACP) represents an exceedingly rare malignant adnexal neoplasm, classified by World Health Organization as the malignant counterpart to Syringocystadenoma papilliferum (SCAP) [1]. First described in 1980, only 78 cases appear in the English literature, predominantly affecting elderly patients with a slight male predominance and favoring the head and neck region, though may appear in atypical sites like perianal area, chest, suprapubic area, etc. [2] These tumors often arise from preexisting SCAP or nevus sebaceus, originating from apocrine or pluripotent appendageal glands, with histopathological features including papillary projections, nuclear atypia, and mitotic activity distinguishing them from benign SCAP. Despite their rarity, SCACP carries metastatic risk—regional lymph node involvement in 22% and distant spread in 6% of cases—necessitating inclusion in differentials for adnexal malignancies to avoid misdiagnosis as benign lesions. [3] This report is about an unfamiliar and giant cystic mass which involved the neck and was successfully managed by transcervical excision.
Case report
An elderly man in his early 90s presented with a 2-year history of a slowly progressive left lateral neck swelling. It began as a small bulge and gradually extended to involve the entire left neck and nape. The painless mass caused marked discomfort and restricted neck movement, impairing daily activities, but there were no speech, swallowing, or respiratory symptoms, no ear or nose complaints, and no significant comorbidities. On examination, a 20 × 20 cm soft, cystic, fluctuant, non-tender, bosselated swelling occupied the left neck, extending from the angle of the mandible superiorly, to just above the clavicle inferiorly, up to 2 cm lateral to midline medially, and to the nape posteriorly (Fig. 1). No scars, nevi, dilated vessels, or signs of thoracic inlet obstruction were seen. The swelling was poorly mobile and inseparable from surrounding musculature, but the trachea and larynx were palpable separately. Oral cavity pharynx, larynx, and cranial nerves were normal.

Lateral neck swelling with anterior, posterior, & oblique view. The star indicates the bosselated, stretched & shiny cystic lesion.
Investigation
The magnetic resonance imaging (MRI) neck of this patient, as illustrated in Fig. 2, showed a large lesion measuring 17 × 13.5 cm on the left side of the neck. The lesion extended posteriorly up to the nape of neck, superiorly abuts the parotid gland and inferiorly extends till the root of the neck. A small portion of the lesion was seen extending between the internal and external carotid artery and the parapharyngeal space on the left side. However, the lesion was lateral to the strap muscles with no extensions into the larynx or pharynx. There were multiple septations and debris seen within this giant swelling with mild T1 hyperintensity. All the above-described features were in favor of a large lymphangioma with the possibility of infection. All other workups were within normal limits, including electrocardiography and 2-D Echo which were done for general anesthesia fitness.
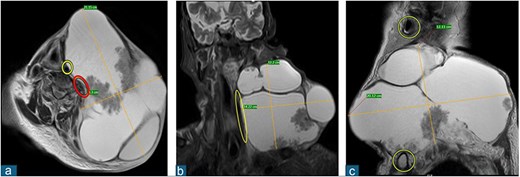
MRI images of the lesion with appropriate sections depicting the extent. (a) Red circle indicates internal jugular vein; yellow circle indicates carotid artery. (b) Yellow circle indicates compressed internal jugular vein. (c) Yellow circles indicate EAC and clavicle.
Treatment
Given the nonspecific clinical and radiological findings, surgery was performed for debulking and symptomatic relief under nasotracheal intubation. Using an elliptical incision around the midportion of swelling (Fig. 3), subplatysmal flaps were elevated to the mass limits. Dissection medial to the sternocleidomastoid exposed the left common carotid artery, Internal jugular vein and vagus nerve; the adherent, thrombosed left internal jugular vein was sacrificed to improve exposure. The left spinal accessory nerve was sacrificed posteriorly. A rent on the cyst discharged black-straw-colored fluid, facilitating shrinkage and dissection of the postero-inferior margin. The giant lesion was excised en bloc, margins freshened and the skin closed in two layers. A 14-French drain was placed. The patient recovered uneventfully, tolerating oral intake from the evening of surgery. A mild left-sided shoulder weakness was noticed & suggested shoulder physiotherapy. He was mobilized early, with daily drain and vitals monitoring, and discharged on day 5 after drain removal. At 8-month follow-up, he remained free of local recurrence (Fig. 9). Histopathology revealed a 560 g (17 × 13.5 × 6 cm) specimen of malignant dermal adnexal tumor consistent with Syringocystadenocarcinoma papilliferum, featuring cystic components, papillary excrescences, hemorrhage, and purulent content. Microscopy showed thick/thin-walled cysts with branching papillary/villoglandular structures, low-grade nuclei, eosinophilic cytoplasm, apical secretions, rare mitoses, psammoma bodies, and stromal microinvasion, with deep invasion but no lymphovascular or perineural involvement; margins (1 mm) were clear (pT3, pN not assigned; AJCC 8th ed.). IHC was CK7/CK19 positive, ruling out common metastases; CK20/TTF-1/PAX8/AMACR/ERG-1/p63/CEA/GATA3/AR were negative, SOX10 weakly positive (Figs 4–8).
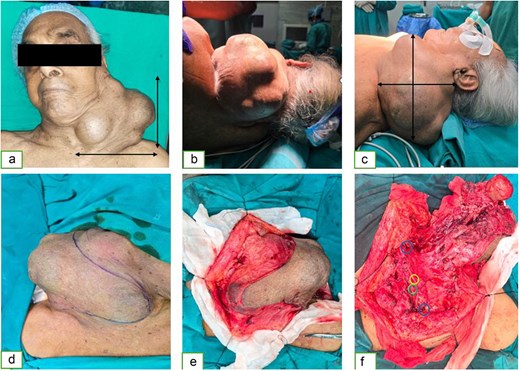
Intraoperative images of the lesion depicting the extent, incision, & relation with vascular structures. (a–c) Gross extent of the lesion. (d) Skin marking over the lesion. (e) Skin flap is raised around the tumor. (f) Relationship of tumor to neurovascular structures of the neck. Blue circles indicate cut ends of IJV; yellow circle indicates vagus nerve; green circle indicates carotid artery.
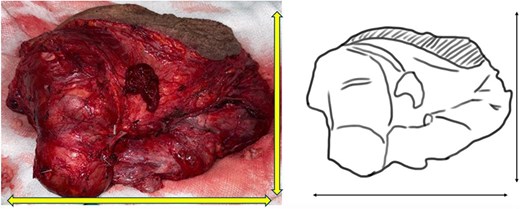
Gross specimen with dimensions. Gross specimen weighed 560 g with exact dimensions of 17 × 13.5 × 6 cm. Additional structures attached – skin ellipse measuring 15.1 × 1.8 cm.
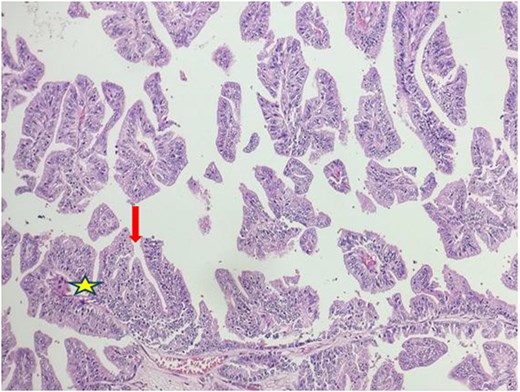
Microscopy showing branching, complex papillary structures with fibrovascular core.
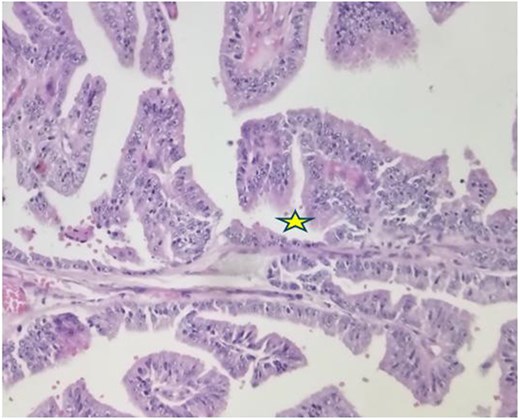
Microscopy showing large areas of superficial epithelium with funnel shaped glandular invagination suggesting dermal origin. The star indicates glandular invagination.
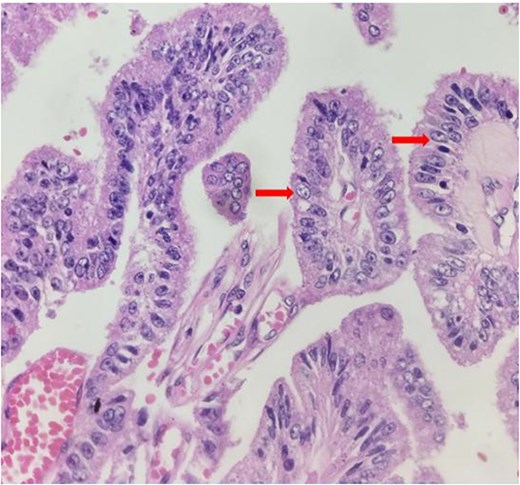
Microscopy showing nuclear atypia and mitotic figures suggestive of malignancy (arrow).
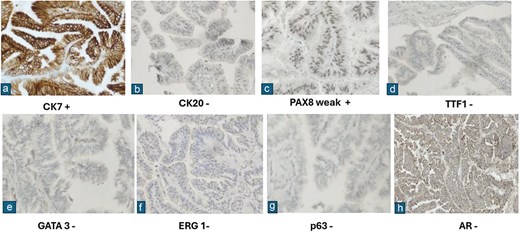
Various results of immunohistochemistry panel.

Follow-up images of the patient after complete wound healing.
Discussion
SCACP is a rare malignant apocrine tumor originating from the pluripotent appendageal glands of the skin. This diagnosis is often preceded by rapid enlargement or ulceration of preexisting nevus or SCAP. This is a tumor so rare that only 78 cases have been reported in the literature. It predominantly affects older men & has a varied presentation such as ulcerated nodule, plaque and rarely non-ulcerative cystic swelling.
A comprehensive literature search including only articles published in English on SCACP of head and neck region using search engines like PubMed and Google scholar identified 44 cases documented till January 2026 (Table 1). Of the reported cases, the median age of presentation was 62.7 years (29–96 years). Majority were males (n = 24;54.5%) & scalp was the most common site, (n = 34/44;75.5%). The neck was one of the less commonly affected sites & reported only in three cases (6.81%). The lease common site among the head and neck region was forehead; only one case has been reported (n = 1/44; 2.27%) The distribution of tumor location within head and neck is shown in Table 2.
List of published literature on SCACP with demographic details, clinical features, & treatment.
| Author, year | Age, y/sex | Location | Size, cm | Duration | Clinical features | Treatment & outcome |
|---|---|---|---|---|---|---|
| Dissanayake & Salm, 1980 [3] | 74/F | Scalp | 6.5 × 5.5 × 3.5 | 30 years | Enlarging exophytic tumor with copious secretion | Excision No recurrence after 6.75y |
| Seco Navedo et al., 1982 [2] | 50/F | Scalp | 6.5 × 6.5 × 2.0 | since birth | with a recent increase in size | Excision Regional lymph node metastasis |
| Bondi et al. [2] 1996 | 47/M | Scalp | 2.5 | Unknown | Solitary ulcerated & crusted | Excision Lost to follow-up |
| Arai et al., 2003 [2] | 64/M | Scalp | 3.5 × 2.5 × 1.2 | 2 years | Enlarged erythematous tumor, surrounded by a bloody crust with a macerated white papule | Excision In situ carcinoma |
| Chi et al., 2004 [2] | 60/M | Ear (auricle) | 4.0 × 4.0 1.0 × 1.0 | Since Childhood | Two verrucous plaques, ulcerated with yellow crusts | Mohs micrographic surgery, no recurrence/metastasis after 6 years |
| Woestenborghs et al., 2006 [2] | 81/F | Scalp | 1.5 × 0.5 | Unknown | Raised tumor with bleeding | Excision SCACP in situ with pagetoid spread |
| Cai et al., 2005 [2] | 32/F | Neck | 1.0 | Since birth | Hyperpigmented, slow-growing verrucous nodule | SCACP in situ |
| Kazakov et al., 2010 [2] | 56/F | Neck | 2.0 × 2.0 | 10 years | Verrucous ulcerated nodule | Excision SCACP in situ |
| Kazakov et al., 2010 [2] | 46/ F | Scalp | 3.5 | Unknown | Ulcerated, foul-smelling neoplasm | Excision SCACP in situ |
| Kazakov et al., 2010 [2] | 67 / M | Scalp | 2.5 | Unknown | Ulcerated nodule | Excision SCACP in situ |
| Kazakov et al., 2010 [2] | 60 / F | Scalp | 3.0 × 2.0 × 1.0 | 30 years | Ulcerated tumor with recent rapid growth | Excision SCACP in situ with pagetoid spread |
| Kazakov et al., 2010 [2] | 81 / M | Scalp | 2.0 | Unknown | Inflammatory plaque | Excision SCACP invasive |
| Kazakov et al., 2010 [2] | 58/ M | Forehead | 2.5 | Unknown | Ruptured cyst | Excision SCACP invasive |
| Leeborg et al., 2010 [2] | 86/ F | Neck | 4.5 × 4.0 × 4.0 | 4 months | Large, erythematous to violaceous, asymmetric, exophytic and discolored lesion | Excision Invasive poorly differentiated Local recurrence seen |
| Aydin et al., 2011 [2] | 67/ M | scalp | 4.0 × 2.0 × 2.0 | Since Childhood | Ulcerative nodular lesion | SCACP invasive No Excision |
| Hoguet et al., 2012 [2] | 86/ M | Eyelid | 0.4 | Unknown | Erythematous, ulcerated, curated nodule | Excision SCACP in situ |
| Bakhshi et al., 2012 [2] | 45/ F | Scalp | 6.0 × 3.0 | 1 year | Hemispherical swelling with rapid growth, granular surface with erosion and crusts, accompanied by satellite lesions | Excision SCACP invasive with spindle cell variant of a sarcoma |
| Arslan 2013 [2] | 66/F | Scalp | 3.0 × 2.2 | 1 year | Well-defined, erythematosus nodular mass | Excision |
| Arslan et al., 2013 [2] | 66/M | Scalp | Unknown | 20 years | Multinodular ulcerated lesions | Invasive 3 regional left cervical lymph node metastasis, radical neck dissection, radiation therapy |
| Peterson et al., 2013 [2] | 65 / M | Scalp | 3.0 × 3.0 | Since birth | Flesh-colored, exophytic tumor with serosanguinous exudate, rapid growth for the last 12 months | Excision SCACP invasive |
| Mohanty et al., 2014 [2] | 80/F | Scalp | 5.0 × 3.3 × 1.3 | 8 years | Friable, exophytic, tan-pink to red | Excision SCACP in situ |
| Castillo et al., 2014 [2] | 32/F | Scalp | 2.2 × 1.7 × 1.5 | Unknown | Solid and cystic tumor with round, yellowish-white in color and with firm consistency | Excision SCACP in situ Local recurrence |
| Satter et al., 2014 [2] | 42/M | Scalp | 4.5 × 4.0 | 1 month | Ulcerated exophytic nodule with satellite papules, easily bled with minor trauma | Excision, posterior neck dissection Lymph node metastasis |
| Parekh et al., 2016 [2] | 74/M | Scalp | 2.0 × 1.8 | Since birth | Enlarging erythematous exophytic nodule with small foci of ulceration | Left neck dissection Lymph node metastasis |
| Chen et al., 2016 [2] | 60/F | Scalp | 2.8 × 2.0 | 1 year | Hairless, rough, ill-defined erythematous erosive warty plaque with serosanguinous exudate | Excision SCACP invasive |
| Zhang et al., 2017 [2] | 64/ M | Scalp | 2.0 | 1 year | Flat verrucous neoplasm | SCACP in situ, mucinous metaplasia. Multiple distant lymph nodes and lung metastasis (died of disease) Excision + radiotherapy |
| Zhang et al., 2017 [2] | 29 F | Scalp | 1.5 | 2 years | Subcutaneous nodule | Excision SCACP in situ |
| Muthusamy et al., 2017 [2] | 78/M | Scalp | 4.5 × 3.5 | 10 years | Ulcerated nodular lesion | Excision SCACP invasive |
| Pagano Boza et al., 2019 [2] | 63/ M | Eyelid | 5.0 × 7.0 | 7 years | Erythematous nodular lesion with ulceration and induration | Exenteration Invasive SCAP Local recurrence |
| Alegria Landa et al., 2019 [2] | 90 / F | Scalp | Unknown | 10 months | Eroded nodule with bleeding | SCACP in situ (death 1 year later from an unrelated cause) |
| McBride et al., 2021 [2] | 68 / M | Scalp | Unknown | Unknown | Mass with skin erosion | N/A |
| Kneitz et al., 2021 [2] | 75 /M | Scalp | 2.5 × 1.8 | Since birth | Nodular mass (growth in 6 months preceding diagnosis) | Excision SCACP invasive |
| Zilberg et al., 2022 [2] | 77/M | Scalp | 0.3 | 3 months | Pearly papule | SCACP invasive Mohs micrographic surgery |
| Cornejo et al., 2024 [2] | 71/M | Scalp | Unknown | Unknown | Unknown | SCACP invasive |
| Cornejo et al., 2024 [2] | 57/M | Scalp | Unknown | Unknown | Unknown | SCACP in situ |
| Cornejo et al., 2024 [2] | 93/M | EAR | Unknown | Unknown | Unknown | SCACP invasive |
| Cornejo et al., 2024 [2] | 66/ M | Scalp | Unknown | Unknown | Unknown | SCACP in situ |
| Cornejo et al., 2024 [2] | 63/ F | Scalp | Unknown | Unknown | Unknown | SCACP invasive |
| Cornejo et al., 2024 [2] | 29 / F | Scalp | Unknown | Unknown | Unknown | SCACP invasive |
| Cornejo et al., 2024 [2] | 64 /F | Scalp | Unknown | Unknown | Unknown | SCACP in situ |
| Cornejo et al., 2024 [2] | 96/M | EAR | Unknown | Unknown | Unknown | SCACP invasive |
| Dupont et al., 2023 [2] | 74 / F | Scalp | Unknown | Since childhood | Slow-growing tumor | SCACP invasive Recurrence on the left conjunctiva Platinum salts and 5-Fluorouracil chemotherapy for 6 months, followed by 3 months chemoradiotherapy |
| Bashinskaya et al., 2023 [2] | 83 / M | Scalp | 1.6 × 1.6 | Several months | Erythematous and tender nodule with hyperkeratotic scale | SCACP invasive Mohs micrographic surgery |
| Verma et al., 2022 [2] | 40 / F | Ear (external auditory canal) | 16.1 × 9.4 × 7.6 | 1.5 years | Polypoidal firm mass with watery discharge | Excision SCACP invasive |
| Present case, 2026 | 94/M | Neck | 17 × 13.5 × 6 | 2 years | Non-ulcerative massive cystic swelling | Transcervical excision SCACP invasive Follow up −8 months no recurrence |
Based on the available literature, distribution of SCACP in head and neck region.
| Location | No. of cases | Percentage (%) |
|---|---|---|
| Scalp | 34 | 75.5 |
| Ear | 4 | 8.8 |
| Neck | 4 | 8.8 |
| Eyelid | 2 | 4.4 |
| Forehead | 1 | 2.2 |
Among the 44 cases, ulceration was the most common presenting symptom (n = 20/44; 45.54%) The tumor size details were available for 32 cases, with an average diameter of 2.85 cm. The duration of presenting symptoms was reported in 27 cases; of these 18 reports provided specific duration. Overall average duration of all these patients was 98.6 months. Interestingly three patients had this tumor since childhood & five of them had since birth.
However, our case is unique in view of unusual presentation i.e. mimicking cystic metastasis & less common site i.e. neck. Despite diagnostic challenges & advanced age our case demonstrates that biological age assessed by G8 geriatric screening tool is a more factor in determining surgical suitability than chronological age, allowing for aggressive management that is both safe and effective. Prompt medical intervention, including imaging and excisional biopsy, remains crucial for a definitive diagnosis. Until now, there are no reliable clinical or histological indicators to determine the prognosis. Further studies on many cases with complete follow-up data are still needed to draw definitive conclusions.
Conflicts of interest
None declared.
Funding
None declared.
Ethics approval
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}