





Abstract
Stapled hemorrhoidopexy (SH) is used for prolapsing hemorrhoids and is associated with less short-term postoperative pain. While constipation is common after SH, proximal sigmoid fecaloma is rarely reported. We report a 49-year-old woman who presented with severe abdominal pain and obstipation 14 days after SH. Although digital rectal examination revealed an empty rectum, computed tomography (CT) demonstrated a large fecaloma in the proximal sigmoid colon, 15 cm proximal to the intact staple line. A rectal tube enema failed, but a targeted high enema via flexible sigmoidoscopy achieved partial softening, followed by successful evacuation with nasogastric polyethylene glycol irrigation. This case highlights that an empty rectum on digital examination does not exclude proximal fecal impaction after SH. Early CT may help differentiate proximal fecaloma from staple-line complications and support stepwise nonoperative management in selected stable patients.
Introduction
Stapled hemorrhoidopexy (SH) is an established option for prolapsing hemorrhoids and, in the early postoperative period, generally results in less pain and lower analgesic requirements than conventional hemorrhoidectomy [1]. Despite this advantage, postoperative constipation and occasional fecal impaction have been reported after SH, whereas fecaloma is only rarely noted in complication summaries [2, 3]. Current guidance for symptomatic hemorrhoids emphasizes practical bowel measures, including adequate fluid intake, increased fiber, and avoidance of straining or prolonged time on the commode [4].
The effect of fiber supplementation is not uniform across patients. Wheat bran can increase stool output and shorten transit in healthy individuals, but constipated patients often have a blunted response, with persistently low stool output and slow transit regardless of bran use [5]. This distinction is particularly clinically relevant in patients with anatomic variants such as dolichocolon, where colonic redundancies are associated with prolonged transit and constipation [6]. In addition, excessive fiber intake has been reported to precipitate fecal impaction/ileus [7]. In patients with impaired propulsion or evacuation, adding stool bulk may promote proximal stool stasis and, in susceptible cases, fecaloma formation. We report a case of proximal sigmoid fecaloma after SH, suggesting a postoperative bowel-regimen–related factor rather than an overt staple-line complication.
Case report
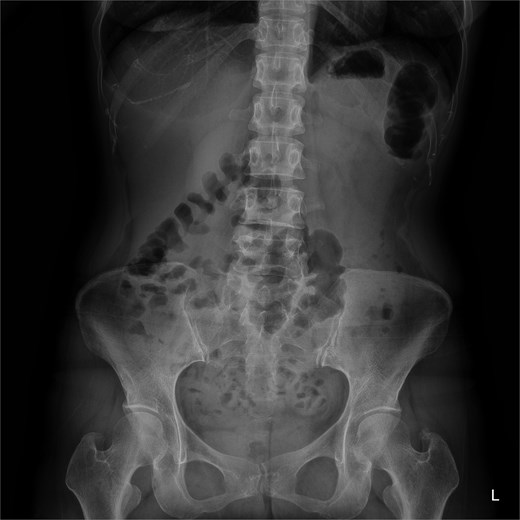
A 49-year-old woman underwent SH with concomitant excision of external hemorrhoids for grade III hemorrhoids. The immediate postoperative course was uneventful, and she was discharged on routine medications, including a bulk-forming fiber supplement. Fourteen days later, she presented with severe abdominal pain and obstipation refractory to oral laxatives and enemas. Physical examination revealed a soft, non-distended abdomen with lower abdominal tenderness. Digital rectal examination demonstrated an empty rectum without evidence of staple-line stricture. Plain abdominal radiography showed extensive fecal loading throughout the colon (Fig. 1). Computed tomography (CT) revealed a large fecaloma in the proximal sigmoid colon, ~15 cm proximal to the staple line, along with marked sigmoid redundancy and tortuosity (Fig. 2).

Plain abdominal radiograph on admission showing extensive fecal loading within the entire colon.
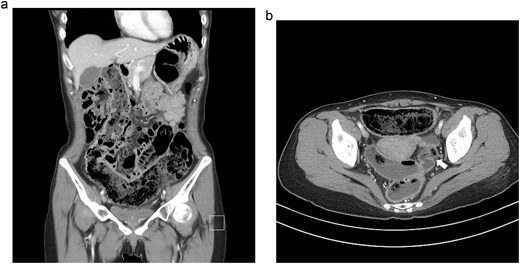
Abdominal CT scans. (a) Coronal view demonstrating a large fecaloma in the proximal sigmoid colon with extensive upstream fecal loading. (b) Axial view revealing the site of acute angulation (white arrow) in the proximal sigmoid colon, ~15 cm proximal to the intact staple line.
A rectal tube enema using 100 ml of glycerin and 400 ml of warm saline failed because the tip could not reach the proximal fecaloma despite full advancement. CT showed no ischemia, perforation, or staple-line complication, and the patient remained clinically stable; therefore, we deferred surgery and pursued a stepwise nonoperative approach. Sigmoidoscopy was technically difficult because of acute angulation of the redundant sigmoid colon, but after traversing the angulated segment, hard impacted stool was visualized in the proximal sigmoid colon (Fig. 3). Glycerin (100 ml) and normal saline (200 ml) were injected directly onto the fecaloma through the endoscopic channel. The patient passed small amounts of hard and liquid stool overnight, and a follow-up abdominal radiograph the next morning showed a clear reduction in fecal burden with partial softening of the remaining stool. To achieve complete evacuation, a nasogastric tube was inserted and 500 ml of polyethylene glycol (PEG) solution was slowly infused over 30 min. This resulted in copious defecation and prompt relief of abdominal pain. A subsequent abdominal radiograph confirmed normalization of the bowel gas pattern (Fig. 4), and the patient was discharged without complications.
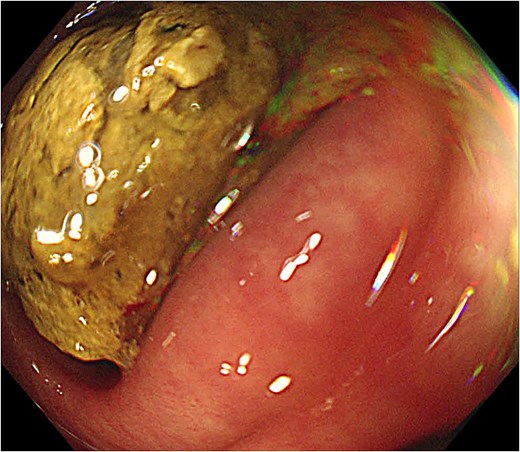
Endoscopic view during sigmoidoscopy revealing hard, impacted stool in the proximal sigmoid colon.
Follow-up abdominal radiograph obtained after completion of nasogastric PEG irrigation. The image demonstrates complete clearance of the fecaloma and normalization of the bowel gas pattern, confirming successful evacuation.
Discussion
Severe fecal impaction after SH is uncommon, but our patient developed a large fecaloma in the proximal sigmoid colon, remote from the staple line. CT showed an intact staple line without stricture or mechanical obstruction, making a technical cause unlikely. The presentation was more consistent with proximal stool retention related to postoperative bulking in the setting of marked sigmoid redundancy.
Fiber supplementation and adequate hydration are commonly recommended to reduce straining [4]. However, in patients with slow transit or colonic redundancy, increasing stool bulk may be less effective and can contribute to proximal stool retention [5, 6]. In this patient, added stool bulk may have pooled in the tortuous sigmoid colon, promoting proximal stasis; bulking agents should therefore be used selectively when impaired evacuation or colonic redundancy is suspected. In a single-center series of stapled anopexy, switching from routine bulking agents to routine lactulose prophylaxis reduced the fecal impaction rate from 7% to 1.4%, supporting an osmotic-laxative approach in patients at risk of stool retention [8].
An important clinical clue was an empty rectum on digital examination. An empty rectum on digital examination may be misleading and does not exclude proximal fecal impaction [9]. Repeated use of laxatives or enemas may partially clear the distal rectum while allowing ongoing proximal accumulation, potentially delaying recognition of high-level impaction.
Management of proximal fecal impaction within a redundant sigmoid colon is challenging. Conventional enemas and digital evacuation may be ineffective when the fecaloma lies beyond the reach of rectal interventions. CT excluded staple-line complications and supported a stepwise nonoperative approach. Endoscopic instillation of glycerin and saline softened the fecaloma and served as a bridge to complete evacuation with nasogastric PEG irrigation. Endoscopic instillation or intra-fecal injection has been described as a nonoperative option for selected cases of refractory fecaloma [7].
In clinical practice, an empty rectum on digital examination can be misleading and does not exclude significant fecal impaction when stool is retained proximally. When a patient presents with obstructive symptoms after SH, early cross-sectional imaging is helpful to rule out staple-line complications and to plan a stepwise nonoperative approach. For patients with impaired evacuation or marked sigmoid redundancy, routine bulking agents should be used cautiously, and an osmotic laxative–based regimen with adequate hydration may be a more dependable starting strategy.
Author contributions
Myung Jae Jin (Conceptualization, Data curation, Formal analysis, Investigation, Writing–original draft, Writing–review & editing) and Jaewon Shin (Supervision, Writing–review & editing)
Conflicts of interest
The authors have no conflicts of interest to declare.
Funding
None declared.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.

{kind=link}
{kind=link}
{kind=link}
{kind=link}