





Abstract
The superior mesenteric vein (SMV) typically lies to the right of the superior mesenteric artery (SMA). We report a cadaveric case in which the SMV was positioned directly posterior to the SMA at the pancreatic head level, then crossed anteriorly to assume a left-sided position at the level of the third duodenal portion (D3). This specific configuration has been documented in isolated radiological reports only and has not, to our knowledge, been confirmed in a cadaveric study. The duodenojejunal flexure was in its normal position, establishing this as a primary isolated vascular variant unrelated to intestinal malrotation. Awareness of this variant is particularly relevant during pancreaticoduodenectomy, complete mesocolic excision with central vascular ligation, and radiological interpretation of mesenteric cross-sectional imaging.
Introduction
The superior mesenteric artery (SMA) and superior mesenteric vein (SMV) form the principal vascular axis of the midgut. Under normal conditions, the SMV ascends to the right of the SMA before joining the splenic vein to form the portal vein [1, 2]. Alterations in this spatial relationship—particularly posterior or left-sided SMV positioning—are uncommon and carry significant clinical implications [3, 4].
Computed tomography studies have identified complete inversion of the SMA–SMV relationship in approximately 4% of patients, with this finding variably associated with intestinal malrotation, adjacent neoplastic displacement, or occurring as an isolated variant [5]. Importantly, a normal positional relationship may be retained in up to 29% of surgically confirmed malrotation cases [6], underscoring that vessel position is neither sensitive nor specific for rotational status in isolation and that isolated vascular positional variants constitute a distinct and underrecognized entity.
Herein, we describe a previously undocumented cadaveric configuration in which the SMV was posterior to the SMA at the pancreatic head level and subsequently crossed anteriorly to assume a left-sided position at D3, with normal bowel rotation confirmed.
Case report
This variant was identified during routine educational dissection of a formalin-fixed cadaver (female, born 1940, deceased 2015) at the Department of Anatomy. No prior abdominal surgery was evident. Ethical approval was obtained from the Institutional Review Board.
After reflecting the greater omentum and transverse colon cephalad and retracting the small intestine inferolaterally, the mesenteric vasculature was systematically exposed. At the pancreatic head level, the SMV was found directly posterior to the SMA—contrary to its expected right-sided position. At the level of D3, the SMV crossed anteriorly over the SMA and transposed to its left side before continuing within the mesentery (Fig. 1). SMA diameter measured 7.79 mm at the level of the pancreatic head. No SMV duplication, anomalous arterial branching, or other vascular abnormalities were identified. The duodenojejunal flexure (angle of Treitz) was confirmed in its normal left-sided position, excluding concurrent intestinal malrotation.
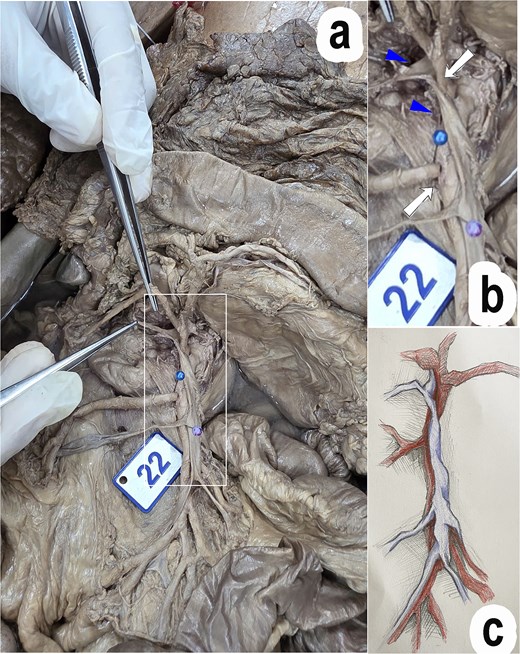
Anatomical variation of the superior mesenteric vessels. (a) The SMV crossing anteriorly and shifting to the left of the SMA at the level of D3. (b) Magnified view. (c) Schematic illustration. Arrows: SMA, arrowheads: SMV.
Table 1 compares the present case with the classical description and previously reported variants.
Comparison of the present case with the classical anatomical description and published SMV–SMA variants.
| Author | Year | Study type | N | Variant | Key findings | Malrotation |
|---|---|---|---|---|---|---|
| Negoi et al. [3] | 2018 | Systematic review | >1000 | Variable SMV position | Majority right-sided; rare positional anomalies | Not specified |
| Ignjatovic et al. [4] | 2004 | Cadaveric | 30 | Venous trunk variation | Gastrocolic trunk focus; positional variation noted | Not reported |
| Applegate et al. [6] | 2006 | Radiological | Pediatric series | SMV inversion | Often associated with malrotation | Yes—associated with malrotation in majority |
| Choi et al. [7] | 2016 | Imaging | 33 | Multiple SMV positions | Right/left/ventral/dorsal positions | Variable; situs anomaly cases included |
| Guo et al. [8] | 2023 | CT study | 115 | DSMV | DSMV in 19.1%; left SMV trunk crossing ventral to SMA in 63.6% | No malrotation—primary vascular variant in colorectal cancer patients |
| Alghamdi et al. [9] | 2024 | Case report | 1 | SMV left of SMA | SMV located left of SMA | Not reported |
| Present study | 2026 | Cadaveric | 1 | Posterior → anterior crossing → left shift | Rare combined dynamic variant; normal bowel rotation confirmed | No malrotation—isolated vascular variant |
Discussion
The SMV was posterior to the SMA at the pancreatic head and left-sided at D3 [10]. This specific combination of posterior positioning followed by distal anterior crossing constitutes a previously undescribed configuration in the cadaveric literature.
Two distinct categories of SMV positional variants exist. The first comprises inversion in the context of intestinal malrotation or situs anomaly, where inverted SMV has ~80%–90% sensitivity for malrotation on sonography [5, 11] but limited specificity—a normal SMA–SMV orientation may be retained in up to 29% of surgically confirmed malrotation cases [6], and inversion does not reliably predict malrotation in situs ambiguus [7]. The second category—to which the present case belongs—comprises primary isolated vascular variants arising from aberrant vitelline venous remodeling, independent of rotational embryopathy. The confirmed normal position of the duodenojejunal flexure and absence of Ladd’s bands establish this distinction; unlike malrotation-associated inversion, this category does not predict midgut volvulus risk.
Left-sided SMV occurs in approximately 0.2%–1.0% of individuals [3]. Guo et al. reported a displaced SMA–SMV relationship (DSMV, as defined by the authors) in 19.1% of 115 patients without malrotation, with the left SMV trunk crossing ventral to the SMA in 63.6% of DSMV cases [8], confirming that aberrant SMV courses can arise as primary vascular variants.
This variant has direct surgical and radiological implications. Three specific operative contexts warrant consideration.
In pancreaticoduodenectomy, the retropancreatic tunnel is created anterior to the SMV–portal confluence. A posteriorly positioned SMV displaces this landmark, and the anterior crossing at D3 may complicate SMV–portal axis skeletonization; preoperative multidetector computed tomography (CT) with 3D reconstruction is essential [6].
In complete mesocolic excision with central vascular ligation for right colon cancer, the right lateral wall of the SMV guides D3 lymphadenectomy. A left-lateralized SMV compresses the working corridor between the SMV and SMA and may obscure ileocolic and right colic artery origins, increasing the risk of inadvertent SMA injury.
Radiologically, posterior SMV at the pancreatic head may be missed on axial CT, and left-shifted SMV at D3 may be misinterpreted as malrotation. Multi-level SMA–SMV assessment combined with evaluation of bowel rotation status is essential.
Conclusion
We report a rare SMV–SMA positional variant involving proximal posterior positioning and distal anterior crossing with leftward transposition. The confirmed absence of intestinal malrotation establishes this as an isolated primary vascular variant, distinct from the well-described malrotation-associated SMA–SMV inversion. Recognition of this pattern is essential for avoiding vascular injury during pancreatic and mesenteric surgery and for accurate preoperative imaging interpretation.
Author contributions
D.L.M.: data collection. D.N.H.: data collection. V.V.U.: manuscript writing. V.N.H.: manuscript writing. H.B.N.: manuscript writing and editing. D.L.M. and D.N.H. performed dissection and data collection. HBN drafted the manuscript. V.V.U., V.N.H., and H.B.N. revised the manuscript critically. All authors approved the final version.
Conflicts of interest
The authors declare no competing interests.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
This study was conducted in accordance with institutional guidelines for the use of cadaveric material in anatomical research and education. Ethical approval was granted by the Institutional Review Board in Biomedical Research at the University of Medicine and Pharmacy at Ho Chi Minh City (Decision No. 520, 27 March 2024).

{kind=link}