





Abstract
Ileo-ileal knotting is a rare, life-threatening cause of small bowel strangulation. Preoperative diagnosis is challenging, and hemorrhagic ascites in reproductive-age women may mimic gynecologic emergencies. A 33-year-old Ethiopian female presented with sudden abdominal pain, vomiting, obstipation, and hemorrhagic shock. Ultrasonography showed dilated small bowel loops and echogenic free fluid, suggesting ruptured ovarian cyst. Due to instability, computed tomography was omitted. Emergency laparotomy revealed 2000 ml of hemorrhagic ascites with normal ovaries and no gynecologic bleeding. An ileo-ileal knot with 180 cm of gangrenous bowel was found; hemorrhagic ascites resulted from transmural ischemia with venous congestion. The gangrenous segment was resected, and stoma created. Short bowel syndrome ensued. Staged jejuno-ileal anastomosis was performed 1 week later with good recovery. This case confirms that hemorrhagic ascites in women does not exclude intestinal strangulation. Early surgical exploration is lifesaving when closed-loop obstruction is suspected.
Introduction
Ileo-ileal knotting is a rare, life-threatening obstruction in which one ileal segment wraps around another, causing rapid vascular compromise and ischemia. It is among the rarest intestinal knotting types and carries mortality rates up to 50% when diagnosis is delayed [1, 2]. Its rarity and nonspecific presentation hinder preoperative recognition.
In low- and middle-income countries, small bowel volvulus is recognized, but ileo-ileal knotting remains underreported [3, 4]. Patients typically present with sudden abdominal pain, vomiting, distension, and obstipation, progressing quickly to ischemia and shock from venous congestion and hemorrhagic ascites [5]. In reproductive-age women, this presentation may mimic ruptured ovarian cyst or ectopic pregnancy.
Radiologic evaluation may be limited in unstable patients. Although computed tomography (CT) improves detection of volvulus and knotting, it is often not feasible in emergencies [6]. Diagnosis is therefore usually intraoperative. A broad differential and high suspicion are essential when hemorrhagic peritoneal fluid is present without a clear gynecologic source.
We report a case initially managed as ruptured ovarian cyst based on clinical and ultrasonographic findings. It highlights diagnostic overlap between surgical and gynecologic emergencies and the importance of early exploration in unstable acute abdomen. This case is reported in accordance with the SCARE guidelines [7].
Case presentation
A 33-year-old Ethiopian female with no chronic illness presented with 9 h of sudden severe periumbilical pain, repeated vomiting, and inability to pass feces or flatus. She had no prior surgery, trauma, or similar episodes. Menstrual history was regular.
She was critically ill with hypovolemic shock: blood pressure 75/45 mmHg, pulse 138 beats/min, respiratory rate 30 breaths/min, pale with cold extremities. The abdomen was distended with infra-umbilical tenderness and guarding; bowel sounds were hypoactive.
Laboratory tests showed anemia (hemoglobin 8.1 g/dl) with normal electrolytes. Urine hCG was negative. Ultrasonography demonstrated markedly dilated small bowel loops with reduced peristalsis and significant echogenic free fluid suggestive of hemorrhagic ascites. Given pelvic hemorrhagic fluid in a reproductive-age woman, ruptured ovarian cyst with hemorrhagic shock was suspected.
Ultrasound-guided paracentesis yielded pure hemorrhagic fluid without bile, feculent material, or pus (Fig. 1). Because of instability, CT was not performed. She was resuscitated with crystalloids, noradrenaline, and four units of packed red cells before urgent laparotomy.

Ultrasound guided tap of the peritoneal fluid, hemorrhagic.
Approximately 2000 ml of hemorrhagic ascites was encountered. Both ovaries, uterus, and adnexa were normal, excluding gynecologic bleeding.
Further exploration revealed extensive small bowel pathology. About 180 cm of gangrenous intestine was identified, beginning 80 cm distal to the ligament of Treitz and extending to 15 cm from the ileocecal valve (Fig. 2). A complex ileo-ileal knot was present: roughly 25 cm of distal ileum tightly rotated 360° around 155 cm of proximal ileum, causing complete obstruction and severe vascular compromise (Fig. 3). The bowel was congested, edematous, and nonviable with hemorrhagic discoloration; the ileocecal valve along with 10–15 cm of the terminal ileum was preserved and no perforation was found (Fig. 4).

Distended frankly gangrenous ileal loop before purse string suture decompression.
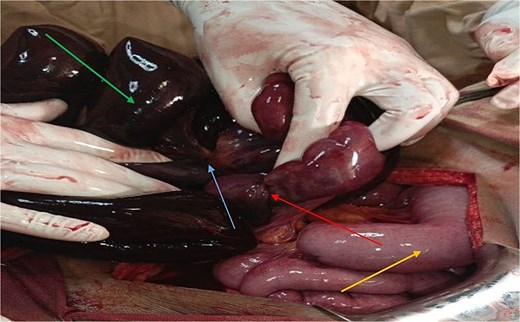
Shows an active component of the distal gangrenous ileum with purse-string suture applied (red arrow) entangled on 360° counter clockwise rotated 155 cm of gangrenous ileum (green arrow) with a knot (blue arrow). The yellow arrow shows the viable segment of the bowel proximal to the most proximal gangrenous ileum.

Shows viable segment of distal ilium over the proximal ascending colon (blue arrow).
Hemorrhagic ascites was attributed to transmural ischemia with venous congestion and serosal bleeding rather than arterial or gynecologic sources. The gangrenous segment was resected. Given limited remaining bowel and critical condition, primary anastomosis was deferred and an end-loop (Hybrid) stoma fashioned, to assess the viability of the bowel ends and as the patient was in shock, leaving a stump of ileum had some risk of stump blowout, and also for the ease of subsequent reconstruction with extracorporeal approach without entering the abdomen midline. Type I short bowel syndrome was diagnosed based on residual length.
Postoperatively, she was managed in a high-dependency unit, kept nil per os (NPO) until the shock was corrected, and received intravenous antibiotics, fluids, electrolyte replacement, and nutritional support. By postoperative day 3, high-output stoma (2.5–3.0 l/day) developed, though electrolytes gradually normalized. After stabilization and given preserved ileocecal valve, intestinal continuity was restored 1 week later via jejuno-ileal anastomosis. Recovery was uneventful with improved oral tolerance. She was discharged stable, and follow-up showed recovery without persistent short bowel syndrome.
Clinical timeline
0 hours (Presentation)—A 33-year-old female presented with sudden onset severe periumbilical abdominal pain, repeated vomiting, and obstipation of 9 h duration.
At admission—Patient was in hypovolemic shock: BP 75/45 mmHg, pulse 138 bpm, RR 30/min, with abdominal distension, tenderness, and guarding.
Initial investigations—Hemoglobin 8.1 g/dl; urine hCG negative. Ultrasound showed dilated small bowel loops and significant echogenic free fluid suggestive of hemorrhagic ascites.
Early diagnostic impression—Suspected ruptured ovarian cyst with hemoperitoneum due to presence of pelvic hemorrhagic fluid in a reproductive-age woman.
Immediate intervention—Ultrasound-guided paracentesis confirmed hemorrhagic fluid. Resuscitation initiated with IV fluids, vasopressors (noradrenaline), and transfusion of 4 units packed red blood cells.
Emergency surgery (same day)—Due to hemodynamic instability, emergency laparotomy and End-Loop stoma performed without CT imaging.
Intraoperative findings—~2000 ml hemorrhagic ascites; normal gynecologic organs. Identified ileo-ileal knot with ~180 cm gangrenous small bowel and only 90 cm aggregate small bowel length viable due to 360° volvulous in association with the ileo-ileal knot.
Definitive management—Resection of gangrenous bowel segment and creation of end-loop (hybrid) stoma. Diagnosis of short bowel syndrome established.
Postoperative course (Days 1–3)—Managed in high-dependency unit with IV fluids, antibiotics, electrolyte correction, and nutritional support. Developed high-output stoma (2.5–3.0 l/day).
Postoperative course (Day 7)—After stabilization, underwent staged jejuno-ileal anastomosis restoring bowel continuity.
Outcome and follow-up—Uneventful recovery, improved oral intake, discharged stable. Follow-up showed good recovery without persistent short bowel syndrome.
Discussion
Ileo-ileal knotting is an exceptionally rare cause of closed-loop strangulating small bowel obstruction, carrying high morbidity due to rapid progression to gangrene. Unlike the more common ileosigmoid knot, this variant is seldom recognized preoperatively [2, 4].
Small bowel obstruction may be simple, strangulated, or closed-loop. Closed-loop obstruction, as in volvulus and knotting, is most dangerous, causing rapid pressure increase, vascular compromise, and necrosis [8, 9]. In developing countries, volvulus and knotting account for a greater proportion of strangulated obstruction than in high-income settings [3].
A major diagnostic challenge in this case was the 2000 ml of hemorrhagic ascites, initially suggesting ruptured ovarian cyst. Intraoperative findings excluded a gynecologic source. Hemorrhagic ascites in strangulating obstruction results from early venous outflow blockage causing congestion and capillary leakage, followed by transmural ischemia with microvascular disruption and serosal bleeding [1, 5]. Large volumes may accumulate without an arterial source, mimicking gynecologic hemorrhage.
Preoperative diagnosis remains difficult due to nonspecific symptoms and rapid deterioration. In reproductive-age women, pelvic hemorrhagic fluid may misleadingly suggest gynecologic emergencies, especially where advanced imaging is limited [4]. CT can demonstrate the “whirl sign” and mesenteric twisting, but instability often prevents its use [6]. Hemorrhagic ascites should not exclude intestinal strangulation.
Management depends on bowel viability. Viable bowel may be untied, though recurrence is rare. In gangrene, resection is mandatory. The choice between primary anastomosis and stoma depends on physiological status, contamination, and residual bowel length [10].
Our patient required extensive resection, resulting in short bowel syndrome, which is defined by inadequate functional small intestine to maintain nutritional and fluid balance, commonly occurring when less than 200 cm of small bowel remains [11]. Preservation of the ileocecal valve improves absorption and slows transit, contributing to favorable recovery in this case.
This case reaffirms that ileo-ileal knotting is a surgical emergency; hemorrhagic ascites may originate from ischemic bowel; and early exploration is lifesaving.
Conclusion
Ileo-ileal knotting is a rare but catastrophic closed-loop obstruction rapidly progressing to ischemia, hemorrhagic ascites, and shock. In reproductive-age women, hemorrhagic intraperitoneal fluid may initially suggest gynecologic emergencies. As shown here, ascites may instead arise from severe bowel ischemia with venous congestion and mucosal extravasation.
When imaging is limited in unstable patients, maintaining a broad differential in acute abdomen is critical. Early surgical exploration remains essential and lifesaving when strangulation is suspected. Assessment of bowel viability and preservation of the ileocecal valve are key determinants of outcome. Prompt recognition, aggressive resuscitation, and timely surgery reduce morbidity and mortality. Increased awareness may prevent diagnostic delay and improve outcomes in patients presenting with hemorrhagic ascites [3].
Highlights
1Ileo-ileal knotting is an uncommon cause of intestinal obstruction that can lead to severe complications if not addressed quickly.
The case of a 33-year-old Ethiopian woman illustrates the difficulty in diagnosing ileo-ileal knotting, which can mimic other conditions like ruptured ovarian cysts.
Management required an exploratory laparotomy, leading to bowel resection and stoma creation due to extensive ischemic changes in the small bowel and hemodynamic instability.
This case highlights the necessity of a broad differential diagnosis in women of reproductive age with acute abdominal symptoms, as prompt intervention is vital for better patient outcomes.
Author contributions
All authors meet the criteria for authorship as recommended by the International Committee of Medical Journal Editors (ICMJE). Eyob Ayenew Engidaw: Case conceptualization, study design, patient management, surgical intervention, data collection, manuscript drafting, and final approval of the version to be published. Kinfemicheal Tilahun Yigzaw: Manuscript drafting, and critical revision of the manuscript. Bethlehem Aliye Asfaw: Critical revision of the manuscript. Eyosias Mesfin Belayneh: Manuscript drafting and review. Alemu Demeke Yehuala: Surgical assistance, clinical follow-up, and management. Cheru Lilay Gebrehiwet: Surgical assistance, clinical follow-up, and management. All authors have read and approved the final manuscript and agree to be accountable for all aspects of the work.
Conflicts of interest
None declared.
Funding
None declared.
Informed consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.

{kind=link}
{kind=link}
{kind=link}
{kind=link}