





Abstract
A 44-year-old male patient presented with persistent ulcer in lower right premolar region. The ulcer was preceded by a swelling which have been misdiagnosed as an abscess and managed by incision and drainage leading to non-healing ulcer. The ulcer managed by excision of the ulcer and complete enucleation of the attached lesion from the bony defect with curettage and reconstructed by bone regeneration procedure and final diagnosis was ameloblastoma. Ameloblastoma management starts from simple enucleation and curettage for small lesion to massive resection with safety margin which needs advance surgery for reconstruction of the mouth to restore normal function. What is unique in this case is regeneration of the defect by particulate bone graft and membrane as none of the reported literature utilized the same technique. Healing went uneventful. Patient resumed normal life activity within 2–3 weeks post-operatively ensuring a good quality of life with no sign of recurrence after 1 year.
Introduction
Ameloblastoma (AM) is a benign but locally infiltrative epithelial odontogenic neoplasm of the jawbones characterized by ameloblast-like cells and stellate reticulum [1]. It is the second most common type tumor of odontogenic origin after odontomas [2]. Clinically, AM is classified into solid/multicystic AM, unicystic AM, and peripheral AM [1]. It has a slight male predilection, with most cases affecting patients between 40 and 50 years old with a predilection for the posterior mandible [2, 3] however, unicystic AM is usually diagnosed at a younger age [2]. Clinically, AM presents as a painless, slow-growing mass that can reach a large size if not treated. Additionally, it can displace and loosen teeth, expand and perforate the cortices, and ultimately cause disfigurement and risk adjacent vital structures [1]. Radiographically, AM presents as a multilocular lesion with a soap bubble or honeycomb appearance with a well corticated margin [1]; however, unicystic AM presents as a unilocular radiolucency with a well-demarcated radiopaque border. Histologically, AMs present peripheral basophilic columnar cells with reverse polarity with the stellate reticulum [2]. Most patients with solid AMs undergo surgical resection, with some patients undergoing enucleation [2], with a recurrence rate of 16% [2]. Herein, we report a case of ameloblastoma in a 44-year-old male patient whose primary clinical presentation was a persistent oral ulcer.
Case study
A 44-year-old male patient presented to the periodontal department at Alahsa Dental Center with a chief complaint of painless swelling on his lower left side for 6 months. The patient had a lesion in the same location previously diagnosed as a dental abscess elsewhere and managed by incision and drainage. The extraoral examination was unremarkable, with no palpable lymphadenopathy. During the intraoral examination, an ulcerative growth of ~8 mm by 8 mm was observed between the mandibular left canine and the 1st premolar (Fig. 1). No deep periodontal pockets were observed on the adjacent teeth, while the results of cold tests, percussion, and palpation were within the normal limits. A well-defined radiolucent lesion was noticed between the mandibular left canine and the 1st premolar with root deviation without evidence of root resorption (Fig. 2). Our differential diagnoses included lateral periodontal cyst and odontogenic keratocyst. Surgically, a sulcular incision from the mesial of the canine to the mesial of the 1st molar with one vertical releasing incision in the mesial to the canine extending beyond the mucogingival junction was made. Full-thickness flap reflection was performed, along with the removal of the lesion between the canine and first premolar, followed by curettage and perpherial osteotomy and osteoplasty of the site. Regeneration of the defect by allograft bone particles (LifeNetHealth ID: 2319784–3016, Code: MD050) covered by a collagen membrane (OsseoGuard Flex Ref: OGF2030, LOT: BDMU22E1) followed by flap adaptation and suturing with 5/0 silk suturing materials (Fig. 3). Histopathologic examination revealed sheets and follicles of odontogenic epithelium within a fibrous stroma. These sheets and islands were characterized by tall columnar basal cells with reversed nuclear polarity (ameloblastoma-like cells) and by loosely arranged stellate-like cells displaying squamous metaplasia, keratinization, and cystic degeneration. Based on that, the diagnosis was ameloblastoma (Fig. 4). Healing was uneventful. The patient was informed about the result and the high risk of recurrence. Despite this, he declined additional intervention and opted for regular follow-up visits. The patient has been under observation for over a year, showing no signs or symptoms of recurrence (Fig. 5).
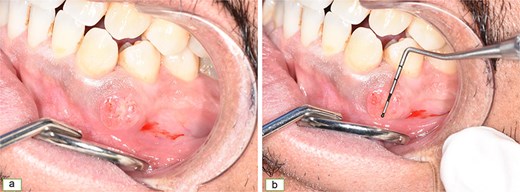
Ulcerative nodular lesion between the roots of the lower left canine and first premolar (a, b).
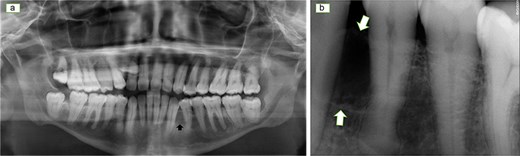
Panoramic radiograph (a) and periapical radiograph (b) showing a unilocular radiolucent lesion between the roots of the lower left canine and first premolar with displacement of the teeth root.

Sulcular incision from the distal surface of the lower left lateral incisor to the mesial surface of the lower left second premolar (a), flap was raised with lesion in place (b), lesion removed (c), and suture in place (d).
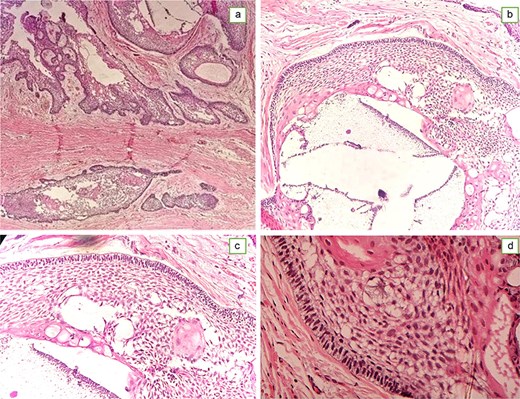
Histological examination showing follicular growth of ameloblastoma like lining with columnar cells with reverse polarity and subnuclear vacuolization and stellate reticulum like cells (a,b).

Follow up visit after 1 year showing bone filling the defect with no sign of recurrence (a,b).
Discussion
In this report, we presented a case of ameloblastoma initially misdiagnosed and treated as a dental abscess, leading to its persistence as a non-healing ulcer. Moreover, we adopted a conservative approach in managing the case by applying a bone graft with collagen membrane.
Ameloblastoma is usually diagnosed based on histological features including the presence of odontogenic islands with tall columnar cells with reverse polarity and stellate reticulum-like cell embedded in fibrous stroma however some radiographic findings could be helpful including presence of a multilocular radiolucent lesion with a soap bubble or honeycomb appearance with a well corticated margin [1]. However, in our case, the radiographic examination posed a challenge and presented as an interdental radiolucency, which made the suspicion of ameloblastoma less likely. In the era of Artificial intelligence (AI), the classical radiographic findings of such a lesion can help achieved a rapid, initial, and accurate diagnosis and avoid improper management. A recent AI-assisted diagnostic tool has utilized cone beam computed tomography (CBCT) and achieved an average score of 79.6% sensitivity, 94.48% specificity, 91.47% accuracy [4]. These are promising result; however, further validation is required and histologic examination remains the gold standard for such cases.
Ameloblastoma rarely manifests as an intra-oral ulcer, and when it does, it is usually associated with a large, aggressive intra-osseous lesion. In contrast, our case involved a small lesion presenting as a persistent ulcer [5, 6].
We managed our patient with conservative management via enucleation and curettage followed by guided tissue regeneration to prevent collapse at the lesion site and used particulate bone graft with no sign of recurrence after 1 year. Ameloblastoma can be managed conservatively by enucleation or through more aggressive approach including resection [2]. However, a systematic review in 2018 compared the recurrence rates between radical and conservative management and found that enucleation had a recurrence rate of 41%, whereas radical approaches have a rate of 8% [7]. Opting for a more conservative approach, as in our case, may lead to a reduction in the negative impact on the patient’s quality of life. The patient was educated about the condition, the possibility of recurrence, and the need for long-term follow-up.
A specific treatment choice should be made with consideration of its impact on patient quality of life in terms of esthetics, function, and morbidity. A questionnaire can be utilized as assessment tool for the impact of certain treatment on patient life quality. Different questionnaire such as oral health impact profile (OHIP-14), self-proposed questionnaire, and university of Washington head and neck cancer questionnaire. Domains to be considered could vary between questionnaires. University of Washington Quality of Life Questionnaire evaluate pain appearance, activity, recreation, swallowing, chewing, speech, shoulder, taste, saliva, mood, and anxiety. At least 6 months of postoperative follow-up and scoring start from zero as worst to 100 as best [8]. In our case, all the domains scored 100 except pain and appearance which was not optimal post-operatively until one week then with follow-up became normal.
Finally, a more conservative approach for ameloblastoma is now being investigated with a recent systematic review reported reduction of ameloblastoma and ameloblastic carcinoma size in 16 out of 17 cases treated with targeted therapy targeting specific target genes with most of whom received dabrafenib [9]. These therapies could reduce the need for extensive surgical procedures and enhance patient outcomes and quality of life; however more research is required to establish standardized treatment protocols and to assess long-term effects on recurrence and quality of life.
Conclusion
Use of guided tissue regeneration procedure to construct residual defect from ameloblastoma could be a promising. This type of management limit intervention to one surgery. It preserved good quality of life health for the patient with one intervention in the dental clinic. Result of treatment was stable up to 1 year of follow up.
Conflicts of interest
The authors hereby declare that there are no potential conflicts of interest with respect to research and publication of this article.
Funding
No funding was received for this project.
Informed consent statement
A written informed consent was obtained for the reporting of this case in a scientific publication.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}