





Abstract
Consequences of Strep A infections can be severe including shock, sepsis, significant tissue destruction, and death. The primary aim of the study was to identify any consistent patterns regarding presentation, patient demographics, and outcomes for patients diagnosed with invasive Strep A infections of the upper limb. A retrospective review of all patients admitted to the plastic surgery department at the Ulster Hospital, Belfast over a 1 year period was conducted. Eighteen patients in total were identified. One third of the patients had documented substance abuse issues. Two thirds of patients needed two or more operative interventions in order to manage their infection. Three patients had digits terminalised (16.6%). Four patients needed tissue coverage following debridement’s, included two skin grafts, one free flap and one pedicled flap. In summation, any individual presenting with a suspected Strep A infection of the upper limb needs urgent review by an appropriate surgical team and vigilant monitoring.
Introduction
Streptococcus, (genus Streptococcus) are a group of gram positive spheroidal bacteria that are a part of the family ‘Streptococcaceae.’ Characteristically these bacteria group together in chains that resemble a string of bead. There are various sub groups that can be classed via various means including colony morphology, hemolysis, biochemical reactions, and serologic specificity. The most common diseases associated with human illness involving streptococci occur primarily in the respiratory tract, bloodstream, or evolve as skin infections. Of these, Group A streptococci would be the most common causative agent [1].
Fortunately, in developed countries Strep A infections resulting in severe sequalae have declined in the last century owing largely to improved living conditions and the availability of antibiotics [2]. However, in 2022, France, Ireland, the Netherlands, Sweden, and the United Kingdom of Great Britain and Northern Ireland, observed an increase in cases of invasive Group A streptococcus disease. It may have been attributable to the post pandemic period where human contact increased and social distancing measures reduced [3] as Group A Strep is usually highly transmissible [4].
For most patients, Strep A infections largely lead to a self-limiting illness such as cellulitis and pharyngitis [5]. However, for the minority that are subject to invasive Strep A, consequences can be severe including shock, systemic sepsis, deep tissue destruction, and transmission of the pathogen can even prove fatal [6]. Unsurprisingly, among patients diagnosed with mono microbial type II necrotising fasciitis Strep A remains most common pathogen [7–9]. When there is severe destruction of skin and soft tissue affecting patient’s limbs the consequences can be devastating and leave individuals with life altering disabilities. Risk factors for such severe infections include male gender, increased age, heart disease, diabetes as well as intravenous drug use [10].
The overall aim for completing this case series was to identify any consistent patterns regarding presentation, patient demographics, and outcomes for those that met inclusion criteria.
A further objective was to raise awareness of the seriousness of these infections in the upper limbs.
Case series
This study was a retrospective review of all invasive Strep A infections of the upper limb that required inpatient admission under the care of plastic surgery in a tertiary referral centre from period June 2022 to May 2023. Data collected included patient demographics, co-morbidities, reason for referral, operations performed, and outcomes. Follow up was between 2 and 14 months.
In total, twenty three patients were identified as having strep infections A, B, C, and G during the time period analyzed. Eighteen of these patients were found to have Strep A as per tissue cultures and were eligible for inclusion in the study. Figure 1 shows cases per month.
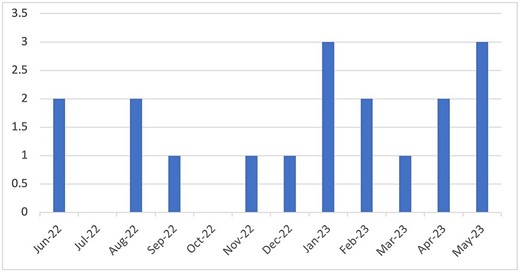
Graph showing the number of Strep A infective cases per month.
Patient demographics
The age range of patient varied from 22 to 77 years old, the average age being 50 years old. There were sixteen males and two females included in the study.
Co-morbidities
Six patients had documented history of substance misuse (33%), either alcohol, drugs, or both. Three patients were diabetic (17%) and three patients were on one or more immunosuppressive drugs for arthritis. These included tocilizumab, methotrexate, hydroxychloroquine, and steroids.
Precipitating events
Three patients could not recall any history of trauma, one individual had an infected mucous cyst and in all other fourteen cases there was a clear history of a trauma to a hand or a visible wound indicating such an event.
Surgical intervention
Only one patient was managed conservatively without surgical intervention. All other seventeen individuals had ‘washouts’ in theater under sterile conditions. The number of ‘washouts’ per person ranged from one to four in total. Overall, two thirds (n = 12) of patients had more than one washout to treat the infection.
Patient outcomes
One patient passed away from an unrelated event. Three patients did not attend surgical follow up or hand therapy. At the time of data collection, four individuals had not been reviewed at outpatients yet. Three patients had a digit terminalized, one reported sensitivity issues and another residual numbness in a digit. One gentleman had DIPJ joint instability, two had notable scar contractures post-surgery. Finally, only two people out of eighteen, reported no long lasting deficits.
Soft tissue coverage post debridement
Four patients required soft tissue coverage post debridement. Two patients needed split thickness skin grafts, one patient required a free flap (medial plantar flap) and one patient was awaiting a dorsal first metacarpal artery flap at time of data collection.
Figures 2 and 3 demonstrate the extent of tissue destruction in an elderly lady with an infected Strep A hand.

Dorsal aspect of a right hand of a 69-year-old female. Strep A infection ensued following a minor laceration during gardening. This is her within 1 week post debridement as an inpatient.

Volar aspect of the right hand of the same patient seen in Fig. 2 (1 week post debridement).
Discussion
In conclusion, the results highlight the seriousness of soft tissue invasive Strep A infections. It is a stark statistic that only one patient was managed conservatively and two thirds of patients required more than one washout. This emphasizes the important of close clinical monitoring of these infections as many patients need multiple debridements in theatre.
Furthermore, out of a total of 18 patients, three individuals had digits terminalized. This is a significant proportion and can leave patients with functional deficits. Aside from these potential disabilities one must also consider it is not uncommon to have psychological repercussions as a result of digit amputation [11].
It is also worth noting that surgical washouts and debridement of necrotic tissue can get source control of a soft tissue infection but antibiotics are also needed in the fight against severe infections. Unfortunately, for future generations and clinicians overseeing such infections, there are more strains of Group A strep emerging that seem to have increased virulence and are less susceptible to antibiotics therapy [12].
Limitations of the study are the small number of patients included and thus it is difficult to make significant inferences. Also, there will be bias regarding patients that may have been managed in outpatient settings by emergency department doctors or in the community by general practitioners. If treated in such a manner it is safe to assume their infection’s had a more indolent course. Furthermore, there is only one plastic surgery unit in Northern Ireland but it is possible that other such infections during the course of the year reviewed were managed by other specialities in different hospitals.
In summation, there are many learning points from this case series. The surgeons encountering such infections acutely need to take a thorough history from the patient and carry out a very detailed clinical examination. A patient may have incurred trauma without their knowledge, or they may have even forgotten about such an event. It is often wise to consult with family members or other persons present with the individual to build up an accurate description of events. Frequently the elderly or those living more chaotic lifestyles may not remember details and this makes it even more important to conduct a thorough exam of the limb to find a potential source for infection. Furthermore, clinicians should have a high index of suspicion for Strep A infection in patients belonging to high-risk groups such as diabetics, immunosuppressed individuals, and intravenous drug users. Once admitted to hospital such patients should reviewed on a regular basis to gage if surgical intervention is necessary as the course can be unpredictable and requires vigilance. Also, liaising with microbiology colleagues is essential to provide optimal care for patients as a dual approach including surgery plus antimicrobials has the best outcomes for patients. Lastly, one should always ensure their colleagues are aware of potential/confirmed admissions of a Strep A infection on a ward so appropriate infection control measures can be implemented according to local hospital guidelines. This can include the use of personal protective equipment (PPE), isolation measures, and patient education re personal precautions. From this perspective, effective communication among colleagues regarding the patients clinical status is imperative to keep staff and other patients safe.
Strep A infections affecting soft tissue of the upper limbs can have catastrophic and devastating consequences for those affected. When there is any suspicion of such a diagnosis, there should be prompt referral to an appropriate surgical team for assessment. Once diagnosis is confirmed these patients should be vigilantly monitored clinically and a multi-disciplinary approach to their management should be adopted, which should include surgeons, microbiologists, and hand therapist at the very least.
Conflicts of interest
The authors declare that they have no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Statement of human and animal rights
This article does not contain any studies with human or animal subjects.
Statement of informed consent
Informed consent was obtained from all individual participants included in the study.
References
Increased incidence of scarlet fever and invasive Group A Streptococcus infection – multi-country (who.int).

{kind=link}
{kind=link}
{kind=link}