





Abstract
Tracheo-innominate artery fistula is a rare but life-threatening complication of tracheostomy, even in chronic cases. A 22-year-old comatose man with a 2-year tracheostomy presented with sentinel bleeding followed by massive hemorrhage. Immediate measures included airway control, digital compression, and fluid resuscitation. Angiography confirmed a 3-mm fistula, and endovascular stenting achieved hemostasis. The patient was extubated on Day 5, with patent stent at 1-month follow-up but remained vegetative. Early recognition of sentinel bleeding and prompt endovascular intervention are critical for survival.
Introduction
Tracheo-innominate artery fistula (TIF) is a rare but devastating complication of tracheostomy, with an incidence of 0.1%–2.3% and mortality exceeding 90% without prompt intervention [1–3]. Typically occurring within 3 days to 6 weeks post-tracheostomy, TIF arises from erosion of the tracheal wall by the tube cuff or tip, leading to fistula formation with the innominate artery [4]. We report a case of TIF in a patient with a 2-year tracheostomy, successfully managed with endovascular stenting, and discuss the challenges in diagnosis and management.
Case report
A 22-year-old comatose man with a history of traumatic brain injury and tracheostomy (placed 2 years prior) presented with intermittent petechial bleeding during tracheal suctioning. He underwent routine cuffed tube replacement under intensive monitoring. Five minutes post-replacement, ~2000 ml of bright red blood erupted from the tracheostomy site, causing hemodynamic instability (systolic blood pressure 70 mmHg, heart rate 130 bpm).
Immediate steps included (i) removal of the tracheostomy tube and orotracheal intubation with cuff hyperinflation to tamponade bleeding, (ii) digital compression of the innominate artery against the manubrium (Utley maneuver) [5], and (iii) aggressive fluid resuscitation (4 units packed red blood cells, 2 units fresh frozen plasma). The patient was transferred to the angiography suite, where computed tomography angiography (CTA) revealed contrast extravasation from the innominate artery into the trachea (Fig. 1). Angiography confirmed a 3-mm fistula at the junction of the innominate artery and trachea. A 10 × 38 mm covered stent graft was deployed via right brachial access, achieving immediate hemostasis. Post-procedure, the patient was extubated on Day 5 and maintained on aspirin (81 mg/day). Neurological examination showed no improvement, consistent with a vegetative state. Follow-up CTA at 1 month confirmed stent patency without endoleak.
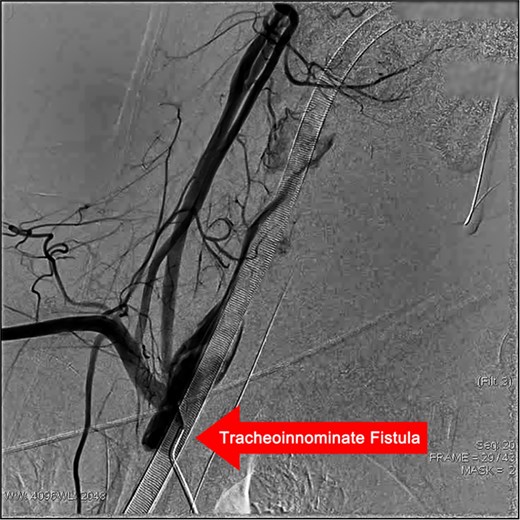
Angiogram of the trachea demonstrating a tracheoinnominate fistula, with contrast medium extravasating from the innominate artery into the trachea through the fistulous tract.
Discussion
TIF is associated with prolonged tracheostomy (>3 weeks), tracheal tube malposition, and cuff overinflation [1]. Our patient’s 2-year tracheostomy duration highlights the need for vigilance even in chronic cases. Sentinel bleeding, observed as intermittent petechiae, occurred 48 hours pre-massive haemorrhage—a critical warning sign present in 43%–65% of TIF cases [6, 7].
Immediate management relies on airway control and hemorrhage tamponade. Cuff hyperinflation and digital compression can temporarily control bleeding in 70% of cases [8]. Endovascular stenting, as used here, offers a less invasive alternative to surgical ligation, with reported success rates of 76% and 30-day mortality of 9% compared to 69% and 40% for open surgery [9]. However, long-term risks include stent infection and migration, necessitating close follow-up [10].
The patient’s vegetative state underscores TIF’s neurological impact, likely due to hypoxic–ischemic injury during haemorrhage. This emphasizes the importance of early recognition and intervention to minimize brain damage.
Conclusion
TIF remains a life-threatening complication of tracheostomy, even in chronic settings. Prompt recognition of sentinel bleeding, immediate airway control, and endovascular stenting are critical for survival. Multidisciplinary collaboration between intensivists, radiologists, and surgeons is essential to optimize outcomes [11].
Conflicts of interest
None declared.
Funding
This work was supported by the Qingdao Medical and Health Outstanding Talent Training Program - Military Characteristic Talent Program (2025–2027).
References
Author notes
Xiangtao Peng, Fangcheng Xu and Lu Gao contributed equally.

{kind=link}