





Abstract
Associated both-column (ABC) acetabular fractures are complex injuries often requiring combined surgical approaches, however this case evaluates the efficacy of an anterior-only technique. A 58-year-old male sustained an ABC fracture after a 3-meter fall, managed via a Pfannenstiel and ilioinguinal first-window approach. Fixation targeted the iliac crest (4.5 mm cannulated screws), comminuted iliac wing (calcaneal plate), and anterior column (reconstruction plate), achieving satisfactory reduction. Posterior fixation was not performed due to satisfactory intraoperative alignment. Pain, function, and quality of life were assessed over 24 months using the Visual Analog Scale (VAS), Majeed Pelvic Score, and SF-12, respectively. Outcomes were excellent: SF-12 Physical Component Summary 56.58, Mental Component Summary 60.76, Majeed Score 91, and VAS 0 at 24 months. This highlights the anterior-only approach’s success in select cases, emphasizing individualized treatment.
Introduction
Acetabular fractures remain among the most complex challenges in orthopedic trauma, particularly when involving the associated both-column (ABC) pattern. These fractures are characterized by their inherent instability and articular displacement, often leading to post-traumatic arthritis if not properly managed [1]. Traditional management has typically required dual anterior and posterior exposures to achieve adequate reduction of these complex fractures [2]. While effective, these extensive procedures carry significant drawbacks, including prolonged operative times, substantial blood loss, and increased soft-tissue complications [3].
In recent years, there has been growing interest in anterior-only approaches for selected ABC fractures. Techniques such as the modified Stoppa and anterior combined endopelvic (ACE) approaches have demonstrated promising results, achieving comparable reduction quality while potentially reducing surgical morbidity [4, 5]. These methods utilize the intrapelvic window to access critical fracture components, often eliminating the need for additional posterior exposure [6].
However, several important questions remain unanswered in the literature. The optimal sequence for fracture fixation—whether to prioritize the anterior column or address both columns simultaneously—continues to be debated [7]. Additionally, clear criteria for patient selection and detailed long-term outcome data are notably lacking [8]. This case report contributes to the growing body of evidence by documenting successful anterior-only management of an ABC fracture, with particular attention to technical considerations and comprehensive 24-month follow-up data [9].
Case report
A 58-year-old male presented following a 3-meter fall, with an isolated ABC acetabular fracture of the right side (Fig. 1). Surgery was performed 2 days after the injury using an anterior pelvic approach via the Pfannenstiel incision combined with the first window of the ilioinguinal approach. Fixation began with the iliac crest using 4.5 mm cannulated screws to anchor the constant fragment, followed by a calcaneal plate to address comminution of the iliac wing, and a reconstruction plate for the anterior column (Fig. 2). As the posterior components were well-aligned post-fixation, a posterior approach was deemed unnecessary. Post-operative after 24 months radiographs and TC demonstrated anatomical reduction with no signs of implant failure (Fig. 3), just as shown in the TC comparison (Fig. 4). The physical exam presents a satisfactory range of motion (Fig. 5). Pain, function and quality of life outcomes were assessed using the Visual Analog Scale (VAS), Majeed Pelvic Score, and SF-12 up to 24 months post-operatively, respectively. The results are summarized in the following table (Table 1) and graphic (Fig. 6).
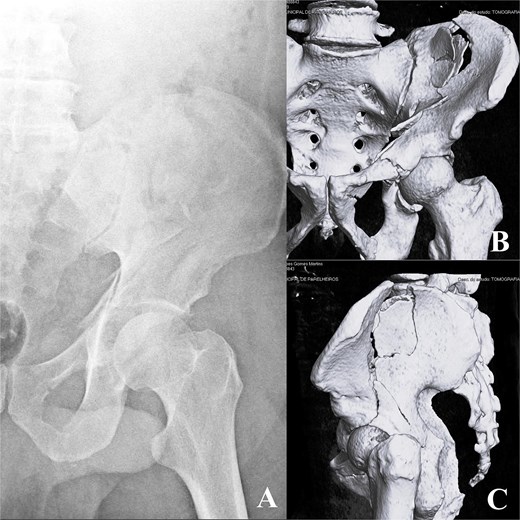
Pre-operative radiograph (A) and computed tomography (CT) scan (B, C).
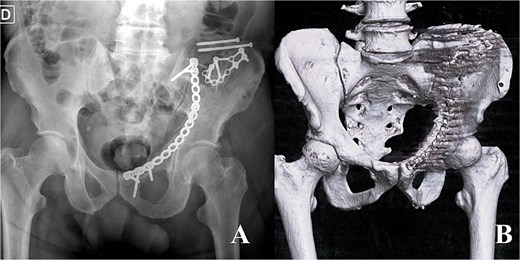
Radiograph immediate postoperative (A) and CT immediate postoperative (B).
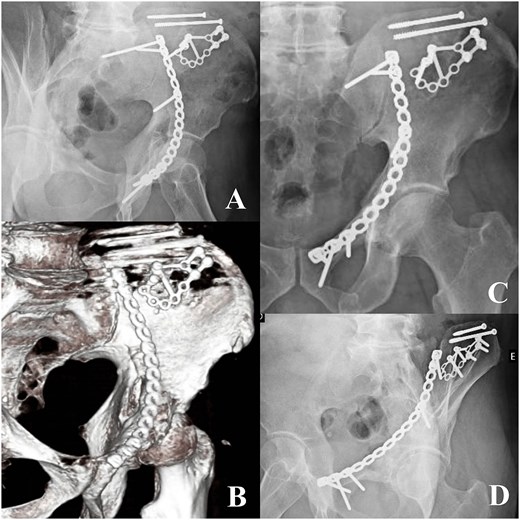
Radiographs 24 months postoperative (A, C, D) and CT 24 months (B).
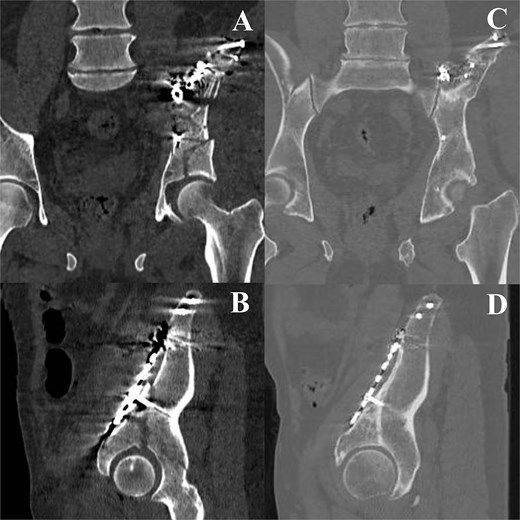
CT immediate postoperative (A, B) comparison with the 24 months follow up (C, D).

24-months follow up hip range of motion.
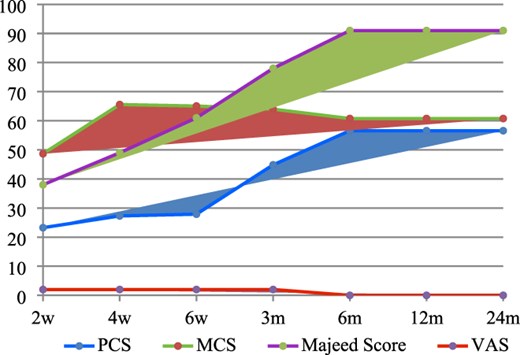
Line graphs comparing outcomes over time.
Score results.
| Interval | PCS | MCS | Majeed score | VAS |
|---|---|---|---|---|
| 2 weeks | 23.25 | 48.67 | 38 | 2 |
| 4 weeks | 27.29 | 65.57 | 49 | 2 |
| 6 weeks | 27.89 | 65.06 | 61 | 2 |
| 3 months | 44.84 | 63.98 | 78 | 2 |
| 6 months | 56.58 | 60.76 | 91 | 0 |
| 12 months | 56.58 | 60.76 | 91 | 0 |
| 24 months | 56.58 | 60.76 | 91 | 0 |
Discussion
The successful management of this ABC acetabular fracture using an anterior-only approach contributes to the growing body of evidence supporting this strategy in select cases [4, 5]. Our experience reinforces that anterior techniques including the modified Stoppa can achieve anatomical reduction while potentially reducing surgical morbidity compared to traditional combined approaches [2, 10]. Consistent with these findings, Chen et al. reported good-to-excellent functional outcomes in 80% of complex acetabular fractures managed through an enhanced anterior intrapelvic approach, frequently avoiding posterior fixation [3]. In our case, the intraoperative assessment of stability after anterior column reduction—a principle validated by recent biomechanical studies [6, 11] —confirmed that posterior elements maintained anatomical alignment following anterior fixation. This outcome aligns with Gänsslen et al.’s documentation of 95.5% anatomical reduction rates using intrapelvic techniques [6].
The fixation sequence employed—beginning with the iliac crest before addressing the anterior column—follows biomechanical principles emphasizing stabilization of reliable fragments first, as described in literature [4, 7]. This stepwise approach proved particularly effective for controlling the characteristic medial displacement seen in these fractures [1, 8]. The patient’s excellent 24-month functional outcomes, including complete pain resolution and high Majeed scores, compare favorably with those reported in larger series of acetabular fractures, irrespective of the surgical approach employed [2].
While our results support anterior-only feasibility, Giannoudis et al. reminds us these techniques require careful patient selection [2]. The intraoperative decision to omit posterior fixation reflects Suzuki et al. emphasis on dynamic assessment, as preoperative imaging alone may not predict posterior stability after anterior reduction [12]. This experience confirms that properly indicated anterior approaches can yield outcomes meeting Matta’s gold standard for anatomical reduction [13].
Unresolved questions include developing reliable preoperative predictors for anterior-only suitability [9] and understanding fixation sequencing’s impact on long-term arthritis risk [7]. Our results, combined with outcomes from ACE and similar anterior techniques [5, 6], suggest these approaches warrant continued study as alternatives to combined exposures. As Raghunathan et al. emphasize, [14] durable functional recovery—achieved here while avoiding posterior morbidity—remains the ultimate measure of success.
Conclusion
This case demonstrates that an ABC acetabular fracture can be effectively managed with an anterior-only approach in selected cases, achieving good radiographic and outcomes over the 24-month follow-up. The individualized approach, supported by safe surgical techniques, underscores the importance of tailoring treatment to the fracture’s complexity. Long-term follow-up confirms stability, with no evidence of complications such as post-traumatic arthritis to date.
Conflicts of interest
None of the other authors have a conflict of interest to declare.
Funding
None of the authors received (or will receive) payments or services, directly or indirectly from companies or scientific funding institutions to support any aspect of this work.
References
Tannast M, Keel MJB, Siebenrock KA et al. . Open reduction and internal fixation of acetabular fractures using the modified Stoppa approach.
Gänsslen A, Staresinic M, Krappinger D et al. . The intrapelvic approach to the acetabulum. Arch Orthop Trauma Surg 2024;145:65.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}