





Abstract
Schistosomal cecum involvement is an extremely rare condition in endemic areas like Sudan. We report a 17-year-old male presenting with acute abdomen diagnosed preoperatively as perforated appendicitis. Emergency surgery revealed purulent peritonitis, a cecal mass, and a large cecal perforation and right hemicolectomy was done. Histopathology revealed viable schistosomal ova and granulomas in the cecum. Post-operative management included anthelmintic therapy. This case presented the third case of large bowel schistosomiasis in Sudan, emphasizing the need for a high index of suspicion for parasitic etiologies in acute abdominal surgical emergencies in endemic regions.
Introduction
Colonic schistosomiasis is an uncommon form of schistosomiasis [1], and diagnosis is usually made by colonoscopy [2]. In Sudan, two cases of schistosomal appendicitis were reported [3, 4] but in this report we present a rare case of schistosomiasis involving the large bowel with perforated cecum confirmed by biopsy findings.
Case report
A 17-year-old Sudanese male presented to our surgical emergency department in August 2025 with a 1-day history of acute, severe abdominal pain. The pain was dull in nature, non-radiating, and non-migratory. Which accompanied by four episodes of large-volume, non-bilious, non-bloody vomiting, also he had nausea and anorexia. The patient had no significant past medical history and no prior surgical operations.
Clinical examination
Upon admission, the patient looks ill. He was anicteric and clinically non-pale. Vitally unstable with tachycardia (116 beats per minute), hypotensive with blood pressure 100/60 mmHg, and significantly tachypneic (respiratory rate reached 40 cycles per minute). Abdominal examination showed tenderness mainly in the right iliac fossa (RIF) with positive rebound tenderness, which indicates localized peritonitis. The bowel sounds were absent; no palpable masses or organomegaly, and no vascular bruits were audible.
Diagnostic investigations
Laboratory investigations on admission showed a total white blood cell count of 7.89 × 109/l (reference range: 4–10 × 109/l), with neutrophilia of 92.6%. Hemoglobin was 11.9 g/dl (12–16 g/dl). All the renal function tests and serum electrolytes were within normal range (urea 20 mg/dl; creatinine 1.1 mg/dl; potassium 4.0 mmol/l; sodium 137 mmol/l). Notably, the C-reactive protein (CRP) level was markedly elevated, which suggests a severe inflammatory process, reaching 196 mg/l (normal range < 5 mg/l).
Ultrasonography of the abdomen and pelvis revealed a structure consistent with a perforated appendix. Otherwise, the liver, spleen, and retroperitoneal organs appeared normal. Based on these clinical and radiological findings, a diagnosis of perforated appendicitis was made.
Surgical management and intraoperative findings
The patient underwent emergency surgical intervention under general anesthesia. Initially, a gridiron incision was performed. Upon reaching the peritoneum, the enteric contents were observed, which necessitated conversion to a midline laparotomy for further exploration.
Intraoperative findings revealed a moderate quantity of purulent and feculent material with minimal contamination limited to the RIF, and inspection to the large bowel identified an anterolateral perforation of the cecum, approximately 1.5 × 1.5 cm in diameter, and located 1 cm from the cecum. In addition to this perforation, thickening of the anterior cecal wall measuring about 4 × 5 cm is also involved the cecum, with diffuse enlargement of the mesenteric and para-aortic lymph nodes (Fig. 1). The liver and spleen appear grossly normal. Given the presence of the mass and perforation, a right hemicolectomy with primary anastomosis was performed done; the operation passed smoothly without complications. The specimen was referred for histopathology to an external laboratory outside because is not available in our hospital.
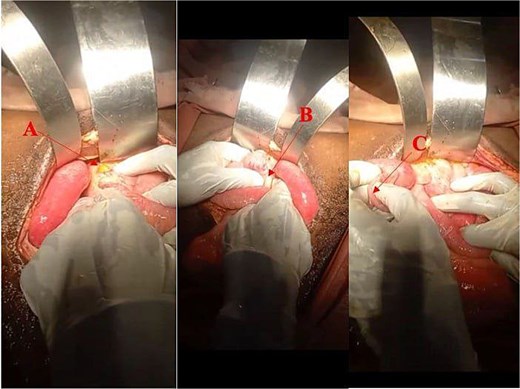
Showing intraoperative findings: (A) Perforated part of the anterior wall of the cecum measuring 1.5 × 1.5 cm; (B) thickened anterior wall of the cecum; and (C) non-inflamed appendix.
Histopathological findings
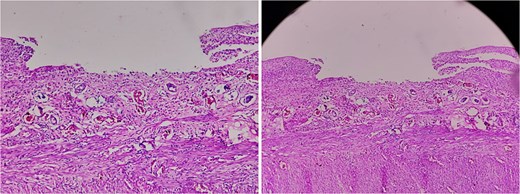
Macroscopic examination of the resected specimen showed a 1.5 cm perforated area in the cecum. The ileum and the ileocecal valve revealed a rough, granular mucosa with ulceration (Fig. 2).
Microscopic analysis revealed a cecal wall with surface ulceration and transmural mixed inflammatory cellular infiltrate. The serosal surface is covered by fibrinous exudates and a mixed inflammatory infiltrate composed of neutrophils, lymphocytes, plasma cells, and histiocytes.
Microscopic analysis revealed a cecal wall with surface ulceration and transmural mixed inflammatory cellular infiltrate. The serosal surface is covered by fibrinous exudates and a mixed inflammatory infiltrate composed of neutrophils, lymphocytes, plasma cells, and histiocytes. The features are those of peritonitis consistent with perforation. Crucially, sections of the appendix revealed several viable schistosome ova associated with histiocytic and giant cell granulomas rich in eosinophils. The features are consistent with schistosomiasis (Fig. 3).
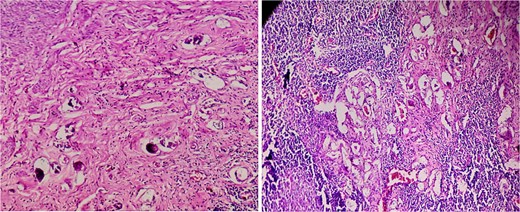
Histopathological specimen of the appendix revealed several viable schistosomal ova associated with histiocytic and giant cell granulomas rich in eosinophils.
Follow-up
Postoperatively, the patient showed rapid clinical improvement. Vital signs stabilized with heart rate 88 bpm; blood pressure 100/70 mmHg, and the respiratory rate 32 cycles per minute. He was managed with NPO, fluid, intravenous antibiotics, and analgesia and was discharged on the eighth post-operative day. At the 2-week follow-up, the patient was in good condition with a clean surgical site. Unfortunately, the patient passed at day 26 before he received praziquantel due to delayed histopathological results in our limited resource setting.
Discussion
Our case reports an unusual presentation of a perforated cecum presenting as acute abdominal pain in a 17-year-old Sudanese man, as a complication of schistosomal infection. While schistosomiasis infection remains a prevalent global disease, it affects over 240 million people annually, especially in sub-Saharan Africa [5]. The species affecting humans are Schistosoma japonicum, S. mansoni, and S. haematobium [6]. Our case highlights the need for putting a high index of suspicion for parasitic etiologies in acute abdominal presentations in an endemic area like Sudan.
Schistosomiasis is a public health burden in our country, Sudan, where it affects a substantial portion of the population, especially children of school age [7]. Despite this high level of endemicity, large bowel schistosomiasis is infrequently reported and documented, for example a systematic review revealed that while the global prevalence of schistosomal appendicitis is about 1.3%, the prevalence in Africa is higher at 2.8%, compared to other areas such as the Middle East, about 0.5% [5]. And they reached 0.1% to 0.2% in non-endemic countries [8]. However, these findings likely underestimate, because of the lack of routine histopathological testing in many resource-limited settings.
Schistosomiasis can affect all segments of the intestine, but the rectum, sigmoid, and descending colon are the main sites in over 90% of cases [9] and can present with polyps, colorectal cancer, ulceration, or erosion of intestinal mucosa and hemorrhoids [2]. The intraoperative finding of a thickened anterior cecal wall and cecal perforation in our patient warrants reporting of the pathophysiological mechanisms involved. In this case, we assume that an untreated ulceration of the cecum due to schistosomiasis had led to this acute presentation of perforation and localized peritonitis.
A major challenge in our case is the diagnosis of intestinal schistosomiasis, because the presentation is indistinguishable from other causes of acute abdomen or peritonitis. Furthermore, the routine investigations provide limited additional information to suggest such etiology. Serological test, and polymerase chain reaction assays, in addition to the presence of eggs in urine or feces, may be used to diagnose when highly suspicious based on risk factors [5]. While colonoscopy is usually used to diagnose intestinal schistosomiasis [2] and CT scans can sometimes reveal pathognomonic “tram-track” calcifications [10], such advanced imaging is not always available or definitive in emergency settings, particularly in low-resource settings. So, the diagnosis relies almost exclusively on histopathological identification of ova.
The surgical management with right hemicolectomy was done due to inability to rule out malignancy [11]. The involvement of the cecum and the presence of a mass mimicking neoplasia often compel more radical resection to ensure source control and rule out malignancy [12]. The standard treatment for all Schistosoma species is Praziquantel [3]. As reported in the literature, surgery treats the complication (perforation/appendicitis), but anthelmintic therapy treats the root cause and prevents recurrence or further systemic complications [13].
In conclusion, our case of large bowel schistosomiasis presenting with perforated cecum illustrates the capacity of a parasitic infection to mimic surgical emergencies. So, in endemic regions such as Sudan, schistosomiasis must be considered a differential diagnosis of any patient presenting with an acute abdomen or atypical bowel masses, and successful management and outcomes depend on a high index of suspicion, combined with surgical management of complications, and with antiparasitic therapy as early as possible. Intestinal perforation due to schistosomiasis is historically extremely rare, making our case a significant addition to the medical literature.
Conflicts of interest
The authors have no conflicts of interest to declare.
Funding
No funding received from any agency.
Ethical approval and patient consent
Written informed consent was obtained from the patient’ guardian for publication of this report and any accompanying images. All identifying data were anonymized.

{kind=link}
{kind=link}
{kind=link}