





Abstract
Malignant transformation of choledochal cysts after internal drainage is a known risk, but presentation nearly four decades later is exceptional. We report a case of cholangiocarcinoma developing 38 years after cystoduodenostomy in a 39-year-old female. Diagnosis was confounded by a periampullary diverticulum, mimicking Lemmel’s syndrome. Multimodal imaging suggested a hilar mass, but endoscopy revealed a large diverticulum. Exploratory laparotomy and frozen section analysis confirmed adenocarcinoma arising from the remnant cyst. The patient underwent complete cyst excision, lymphadenectomy, and Roux-en-Y hepaticojejunostomy. This case underscores two critical lessons: the carcinogenic risk of internal drainage persists indefinitely, necessitating lifelong surveillance; and secondary malignancies can anatomically mimic benign conditions like Lemmel’s syndrome, requiring a high index of suspicion and meticulous surgical management.
Introduction
One of the most concerning complications of choledochal cysts is biliary malignancy, particularly in cases that have not been completely excised or were historically managed with internal drainage procedures, such as cystoduodenostomy [1]. The rate of malignant transformation increases significantly with age and is reported to be much higher in patients with retained cysts compared to those who undergo primary excision. In patients who undergo complete cyst excision, the postoperative risk of malignancy decreases significantly to approximately 0.6%, whereas in those with primary cysts left in situ, the risk remains as high as 9.9% [2].
Numerous studies have investigated the long-term outcomes and carcinogenic risk of choledochal cysts [1, 3, 4]. However, delayed carcinogenesis occurring 38 years after cystoduodenostomy is exceptionally rare. To the best of our knowledge, this is the first such case reported in Vietnam.
This report highlights the critical importance of lifelong surveillance for patients with a history of internal drainage. Furthermore, we discuss specific imaging characteristics to avoid diagnostic pitfalls—particularly the potential to mimic benign conditions like Lemmel’s syndrome—and share our experience in the surgical management of this complex pathology.
Case presentation
A 39-year-old female presented with a one-month history of fever, jaundice, and dark urine. Her medical history included surgery for a choledochal cyst at one year of age (specific method unknown). Physical examination revealed jaundice and fever. Laboratory tests indicated inflammation (WBC 12000/μL; hsCRP 30 mg/L) and obstructive jaundice (Direct/Total Bilirubin: 96/115 μmol/L; GGT 333 U/L). Tumor markers (CA 19–9, CEA, AFP) were normal.
Abdominal ultrasound and CT showed a hilar mass causing biliary obstruction and pneumobilia, initially raising suspicion of hilar cholangiocarcinoma complicated by a fistula (Fig. 1A and B). However, MRCP suggested a duodenal tumor at the D1 – D2 junction invading the biliary tree (Fig. 1C and D). Esophagogastroduodenoscopy revealed a large diverticulum (30 mm) impacted with food debris at the D1-D2 junction, without visible intraluminal tumor. Consequently, Lemmel’s syndrome was considered the primary working diagnosis.
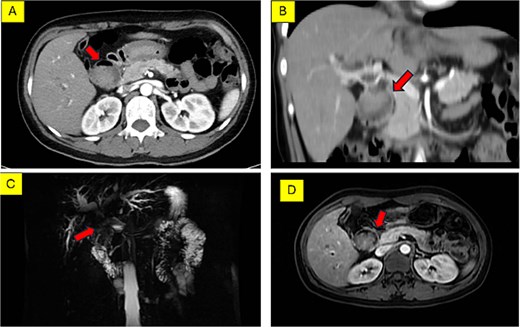
Preoperative imaging of the hilar lesion. (A) Axial MSCT scan showing the mass. (B) Coronal MSCT scan demonstrating the extent of the lesion. (C) 3D reconstruction of the biliary tree indicating the location of the tumor. (D) Axial MRI scan (T1-weighted) of the lesion.
Given the diagnostic uncertainty and progressive jaundice, exploratory laparotomy was performed. Intraoperatively, dense adhesions involving the duodenum and stomach were encountered. Dissection revealed a firm tubular structure (25x50 mm) inseparable from the duodenal bulb and an atrophic gall bladder (Fig. 2A). A wedge resection of the adherent duodenal wall was performed en bloc with the mass. Further dissection identified an atrophic distal bile duct entering the pancreatic head, consistent with a prior cystoduodenostomy (Fig. 2B–D).
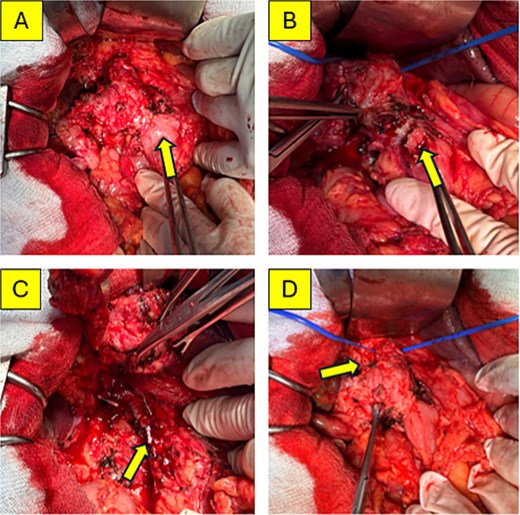
Intraoperative findings. (A) The second portion of the duodenum (D2) densely adherent to the cyst (arrow). (B) The duodenal defect following wedge resection at the site of adhesion. (C) The atrophic distal common bile duct entering the common pancreaticobiliary channel. (D) Dissection of the mass from the portal vein, encircled by a blue vessel loop.
Examination of the opened specimen revealed a dilated cyst containing stones, food debris, and a papillary lesion on the cyst wall (Fig. 3A and B). Frozen section analysis confirmed adenocarcinoma arising from the cyst, with negative resection margins. Reconstruction involved extended lymphadenectomy, primary closure of the duodenal defect, and Roux-en-Y hepaticojejunostomy. A transanastomotic stent was placed. The postoperative course was uneventful; the patient was discharged on Day 7. Final pathology confirmed moderately differentiated adenocarcinoma with negative lymph nodes (0/5) (Fig. 4A and B).
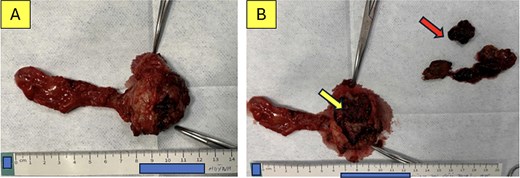
Specimen examination. (A) The en bloc resected specimen. (B) The opened cyst revealing suspicious malignant tissue (lower arrow) and food debris mixed with biliary stones within the lumen (upper arrow).
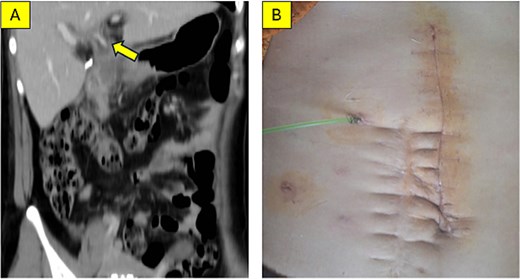
Postoperative outcomes. (A) Coronal MSCT scan at 4 weeks post-surgery; the arrow indicates the transanastomotic stent (catheter) placed via the jejunal limb into the common hepatic duct. (B) Clinical photograph showing the healed incision and the external biliary drain.
Discussion
Choledochal cysts, which demonstrate a marked Asian and female predominance [5, 6], are associated with a grave risk of biliary malignancy, reaching incidence rates of 20%–30% in young adults [2]. Crucially, this carcinogenic risk remains substantial even after internal drainage if the cyst is not completely excised [2, 4].
Malignancy Risk and Pathogenesis The overall risk of malignancy in choledochal cysts is estimated at 10%–15% and increases progressively with age: approximately 1% in the first decade, 15% after age 20, 26% after age 40, and rising to 45.5% in patients over 70 years old. The most common histological types arising from the cysts are adenocarcinoma or cholangiocarcinoma (73%–84%). Tumors may develop within the cyst itself or at other sites in the hepatobiliary-pancreatic system [5].
Regarding pathogenesis, malignant transformation is considered the result of chronic inflammation driven by recurrent cholangitis or the reflux of pancreatic juice due to an anomalous pancreaticobiliary junction. This environment promotes mucosal dysplasia, while biliary stasis facilitates the proliferation of bacteria (e.g. Escherichia coli), which convert bile salts into carcinogens [5]. In our patient, the history of cystoduodenostomy likely established a mechanism for the chronic reflux of not only pancreatic enzymes but also food debris into the biliary tree. This led to stone formation and stasis, serving as the catalyst for biliary carcinogenesis.
Previous studies have emphasized the critical need for long-term surveillance in patients with retained cysts, as the risk of malignancy in the remnant bile duct increases significantly, particularly after a latency period of 15 years [7]. In this case, the malignancy manifested 38 years post-surgery. For patients who have undergone internal drainage (cystoenterostomy), periodic follow–up is mandatory, as the incidence of long-term complications—such as cholangitis, hepatolithiasis, pancreatitis, or malignancy—can reach up to 70% [8].
Diagnostic Challenges Diagnosing malignancy in these patients is challenging because the distorted anatomy can mimic benign conditions. The classic triad of jaundice, abdominal mass, and pain is rare in adults [5]. In our case, the imaging features initially resembled Lemmel’s syndrome—a rare condition characterized by obstructive jaundice caused by a periampullary duodenal diverticulum [9, 10]. As noted in recent literature, distinguishing between a mechanical obstruction by a diverticulum and an infiltrating malignancy requires careful multimodal evaluation [11]. Multi-slice CT and MRCP are essential for delineating these complex anatomical relationships. MRCP is particularly valuable, offering a sensitivity of 90%–100% for diagnosing biliary cysts and visualizing the pancreaticobiliary junction [5].
Management complete cyst excision with Roux-en-Y hepaticojejunostomy is the standard of care to remove the premalignant tissue. While minimally invasive approaches (laparoscopic or robotic) are increasingly performed with excellent outcome, open surgery remains crucial for complex cases involving malignancy and dense adhesions [12]. Our case shares similarities with reports by Baik et al. [1] who described a malignant transformation 35 years after cystoduodenostomy, requiring extensive resection. Similarly, Chaturvedi et al. [3] highlighted the poor prognosis when diagnosis is delayed. Therefore, long-term follow-up is the key to early detection [13].
In the reported case, the ambiguous surgical history combined with altered anatomy presented a significant diagnostic challenge. The possibility of malignant progression on the background of a prior cystoduodenostomy must always be considered, even when tumor markers are normal. A meticulous, step-wise surgical approach is crucial to avoid irreversible injury to major vascular and biliary structures. Furthermore, intraoperative frozen section analysis is indispensable for establishing a definitive diagnosis and ensuring negative resection margins.
In summary, it must be emphasized that complete cyst excision with hepaticojejunostomy remains the gold standard for choledochal cysts. While internal drainage (cystoenterostomy) was historically used or may be considered in rare specific circumstances, strict and lifelong surveillance is mandatory. This is crucial for the early detection and timely management of late complications, particularly biliary malignancy, as demonstrated in this report.
Acknowledgements
We thank the participants who all contributed samples to the study.
Author contributions
Thien Lai Vo had full access to all the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: Hoai Kim Nguyen and Thien Lai Vo. Acquisition of data and surgical performance: Thien Lai Vo and Ho Tran. Drafting of the manuscript: Phuoc Thanh Bui and Thanh Phuoc Cong Nguyen. Critical revision of the manuscript for important intellectual content: Hoai Kim Nguyen. All authors read and approved the final manuscript.
Conflicts of interest
The authors declare that there is no conflict of interest.
Funding
This study has not received any external funding.
Data and materials availability
All data sets collected during this study are available upon reasonable request from the corresponding author.
Informed consent
Written and oral informed consent was obtained from participant included in the study.
Declaration
We hereby certify that this is the original research work of our team. All information presented in this report is truthful and has not been published in any other research project or publication.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.

{kind=link}
{kind=link}
{kind=link}
{kind=link}