





Abstract
Subscapular hematomas are rare entities that pose diagnostic and therapeutic challenges due to their deep anatomical location and nonspecific presentation. Delayed recognition may lead to abscess formation and long-term functional impairment. We report the case of an 18-year-old male who presented with progressive pain, swelling, and restricted range of motion of the right shoulder following blunt trauma. Imaging revealed a large subscapularis hematoma with an associated smaller intramuscular deltoid hematoma. The patient underwent expedited surgical evacuation using a modified dorsal scapular approach with two incisions, allowing safe and effective drainage while preserving surrounding neurovascular structures. A total of 450 ml of hematoma was evacuated. Postoperatively, inflammatory markers declined, pain resolved, and shoulder range of motion improved substantially with physiotherapy. No complications were observed during follow-up. This case highlights the importance of early diagnosis and supports the dorsal scapular approach as a safe and effective option for managing deep periscapular hematomas.
Introduction
Subscapular hematomas are rare, difficult to diagnose due to deep anatomy, and may progress to abscess formation if untreated [1–4]. The surgical approach was adapted from the dorsal subscapularis technique described by Furuhata et al., modified with an additional posterolateral incision to address the concomitant deltoid hematoma [5]. We present a case of an 18-year-old male presenting with subscapular hematoma, demonstrating safe management using the dorsal scapular approach.
Case presentation
An 18-year-old boy presented to our emergency department with history of pain and swelling in his right shoulder with restricted range of movement for the last 2 weeks. He had a history of blunt trauma to the right arm with some heavy object. On examination, the patient had a swelling over the upper arm extending over the shoulder region and pronounced over the scapula along with bruising over the posterior aspect of the axilla. Range of Motion (ROM) was measured using a goniometer, assessing elevation, external rotation, and internal rotation of the affected shoulder. Active shoulder ROM was markedly reduced due to pain (Table 1).
Range of motion pre- and postoperatively: affected and unaffected sides.
| Movement | Preoperative (affected/unaffected) | Postoperative at 2 weeks | Postoperative at 12 weeks |
|---|---|---|---|
| Elevation (°) | 40°/150° | 80°/150° | 140°/150° |
| External rotation (°) | 20°/80° | 50°/80° | 75°/80° |
| Internal rotation (°) | 30°/75° | 60°/75° | 70°/75° |
On palpation, the swelling was tender to touch and passive movements were also limited due to pain and swelling. Pain levels were recorded using a numerical rating scale (NRS), ranging from 0 (no pain) to 10 (worst pain imaginable) and was recorded at 7. Initially, a provisional diagnosis of scapulothoracic dissociation was made and computed tomography (CT) scan was advised. This revealed a large lobulated hematoma in the subscapularis muscle, as shown in the coronal plain CT image (Fig. 1).
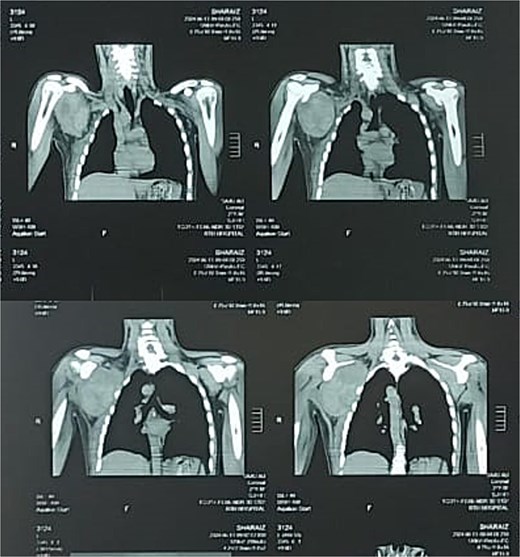
Preoperative coronal plain CT image showing the subscapularis muscle hematoma.
The CT scan showed a larger well defined lobulated hematoma (8.9 × 8.5 × 11.5 cm) in the subscapularis including fluid levels representing hemorrhage. The deltoid showed a smaller hematoma measuring 1.8 × 1.6 × 2.1 cm. Preoperative and postoperative laboratory findings are summarized in Table 2. The patient did not report any co-morbidities or anticoagulative use.
Laboratory findings pre- and postoperatively: trends in hematological and inflammatory markers.
| Parameter | Normal range | Preoperative value | Postoperative (2 days) | Postoperative (2 weeks) |
|---|---|---|---|---|
| WBC count (×103/μl) | 4–11 | 8.9 | 7.5 | 6.8 |
| Hemoglobin (g/dl) | 13.5–17.5 | 11.3 | 8.6a | 12.1 |
| Platelet count (×103/μl) | 150–400 | 210 | 200 | 195 |
| CRP (mg/dl) | <10 | 34 | 11 | 6 |
aIndicates transfusion after surgery.
Although the patient had not yet developed systemic signs of infection, early surgical exploration and drainage was expedited given the size of the hematoma and the risk of hematogenous spread and abscess formation, which has been associated with potentially severe outcomes [2–4]. Under general anesthesia, a modified dorsal scapular approach was employed using two anatomically guided incisions, each targeting a distinct hematoma compartment (Fig. 2).

Preoperative posterior view of the patient showing markings for the two incisions used in the modified dorsal scapular approach: a vertical medial parascapular incision for subscapularis hematoma access and an oblique posterolateral incision for deltoid hematoma drainage.
A vertical medial parascapular incision was made parallel to the medial border of the scapula, through which blunt dissection was carried out through the trapezius and rhomboid muscles to enter the scapulothoracic plane. This allowed safe access to the deep surface of the scapula and evacuation of the large (~300 ml) hematoma within the subscapularis muscle, followed by copious saline irrigation (Fig. 3). A second oblique posterolateral incision was made over the posterior aspect of the shoulder, along the posterior axillary–deltoid region. Although the deltoid hematoma was small on imaging, a deliberate larger incision was employed to ensure adequate drainage, allow thorough inspection for active bleeding, and facilitate identification of any occult pathology. The posterior deltoid fibers were split in line with the muscle, with careful attention to avoid the axillary nerve. Although the CT-estimated hematoma volume was less than 7 ml, its organized and partially congealed nature required copious intraoperative saline irrigation to achieve adequate fragmentation and evacuation, accounting for the ~150 ml of total drainage fluid from this compartment. A closed suction drain was placed within the subscapularis cavity prior to layered wound closure (Fig. 4).

Intraoperative view showing the congealed hematoma in the subscapular region.

Immediate postoperative view showing the suction drain placement and stitched incisions.
The suction drain had around 300 ml/day output for first 2 days and it settled during following days. Drain was removed once output settled, by which time, the wound had healed significantly, as seen in Fig. 5. Physiotherapy was started immediately during post-operative course.

Postoperative view at the time of drain removal showing healing of the surgical site.
Post-op hemoglobin levels were 8.6 mg/dl and one packed red blood was transfused. CRP levels were repeated and they showed decline as well (Table 2).
Postoperative outcomes were encouraging, including a normal ROM and no recorded pain. No notable complications were noted in post-operative period. Follow-up was advised after two weeks for stitch removal then at 6 and 12 weeks. No significant concern was reported.
Discussion
Subscapularis and deltoid hematomas are extremely rare, and standardized management or surgical guidelines remain poorly defined due to the limited number of reported cases. The dorsal scapular approach, as described by Furuhata et al., allows safe and effective drainage while preserving surrounding neurovascular structures [5]. In contrast, Christman-Skieller et al. reported a posterolateral approach for abscess evacuation, which may pose a higher risk of neurovascular injury because of its anatomical trajectory [6]. The dorsal approach was therefore selected in this case to minimize neurovascular risk while achieving complete evacuation. Only a small number of subscapular abscesses have been reported, some with hematogenous spread, underscoring the need for timely drainage [2–4, 7, 8]. Non-traumatic subscapularis hematoma is even rarer, with isolated reports associated with anticoagulant therapy [1, 9]. Delayed or missed diagnosis may lead to chronic complications, such as calcification or ossification, as described by Ladermann and Zelmanovich [10, 11]. Early recognition is therefore essential, as prompt management may prevent progression and, in select cases, allow successful conservative treatment [12, 13].
Previous studies indicate that muscle injury or anticoagulant therapy can lead to the development of intramuscular hematomas, which may initially present as painless swelling or as pain associated with restricted range of motion [2, 9–11]. Because early symptoms can be subtle or nonspecific, diagnosis is often delayed, increasing the risk of progression and functional impairment. These findings highlight the need for heightened clinical suspicion, particularly in patients with a history of trauma or anticoagulant use, to facilitate timely diagnosis and appropriate intervention.
Our study showed that the dorsal approach is safe, with a dual-incision technique within the dorsal scapular approach (one medial parascapular and one oblique posterolateral) effectively draining both the subscapularis and deltoid hematoma compartments while preserving neurovascular structures. Pre- and postoperative metrics for evaluating success included ROM and pain levels. ROM was measured using a goniometer, and pain was assessed using a NRS, consistent with evaluation methods reported in other rare intramuscular hematoma cases involving different muscle groups [10, 13].
In broad terms, surgical approaches to periscapular collections include the anterior deltopectoral approach, the posterolateral approach, and the dorsal subscapularis approach. The deltopectoral approach, while most frequently reported, provides limited access to posterior subscapular collections [14]. The posterolateral approach, as employed by Christman-Skieller et al., risks neurovascular injury due to its anatomical trajectory [6]. CT-guided percutaneous drainage represents a minimally invasive alternative in select cases with early-stage or purely liquefied collections, though it may be inadequate for organized hematomas [15, 16]. The modified dorsal scapular approach employed in this case offered posterior access to both compartments while minimizing neurovascular risk [5]. Nevertheless, timely drainage remains a consistent recommendation to achieve optimal functional outcomes.
Conclusion
Subscapularis and deltoid hematomas are rare clinical entities that require a high index of suspicion for timely diagnosis, particularly following trauma. This case demonstrates that the dorsal scapular approach allows safe and effective evacuation of deep periscapular hematomas while preserving neurovascular structures. Early surgical intervention resulted in marked pain relief and restoration of shoulder function without complications. This approach may be considered a reliable option for managing similar rare presentations to optimize functional outcomes.
Conflicts of interest
None declared.
Funding
The authors received no funding for this work.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}