





Abstract
Epidermoid cysts are benign lesions composed of an epithelial lining filled with keratinous debris. The absence of skin appendages distinguishes them from true dermoid cysts. While they may occur in various anatomical locations, they rarely exceed the 5-cm threshold used to define ‘giant’ lesions. We report a unique case of a giant epidermoid cyst arising from the floor of the mouth, reaching a maximum diameter of 10 cm and initially mimicking a foregut duplication cyst on imaging. We describe its clinical presentation, radiological evaluation, surgical management, and histopathological diagnosis, alongside a review of the current literature.
Introduction
Epidermoid cysts are uncommon lesions of the head and neck, representing 1.6%–6.9% of cases [1]. They may be congenital—arising from developmental anomalies—or acquired through trauma, which results in the implantation of epidermal cells into the dermis and subsequent keratin accumulation. These cysts typically occur in males and present most frequently in the third to fourth decade of life [2].
Their clinical and radiological features often overlap with other midline cystic neck lesions, including thyroglossal duct cysts, plunging ranulas, and pharyngeal cysts such as foregut duplication cysts. The latter represent benign mucosal-lined cysts resulting from abnormal budding of the primitive foregut during embryogenesis. Given the close anatomical relationship between midline epidermoid and pharyngeal cysts, distinguishing between them based on imaging alone can be challenging. As histopathology provides the definitive diagnosis, complete surgical excision remains the standard of care for both entities.
Case report
A 28-year-old woman presented to the head and neck clinic with a 10-year history of a slowly enlarging midline neck mass associated with progressive dysphagia. Her past medical history included asthma and learning difficulties.
Clinical examination revealed a large midline swelling extending laterally into the submandibular spaces, with marked elevation of the floor of mouth and posterior displacement of the tongue. The mass was soft, fluctuant, non-tender, and did not move with tongue protrusion. There were no overlying skin changes and no signs of airway compromise (Fig. 1).

Preoperative facial view showing large midline neck mass.
Ultrasound imaging demonstrated a large, well-defined cystic lesion arising from the floor of the mouth with displacement of the mylohyoid and intrinsic tongue musculature, without internal vascularity (Fig. 2). Fine-needle aspiration yielded cyst contents only, without further diagnostic information.

Ultrasound of neck showing large well defined cystic midline lesion involving floor of mouth.
Magnetic resonance imaging (MRI) of the neck demonstrated a bilobed cystic lesion measuring 10 × 6.3 × 5.8 cm extending through the mylohyoid muscle and elevating the tongue base. The lesion displayed T2 hyperintensity consistent with a cystic structure (Fig. 3). No cervical lymphadenopathy was present. Differential diagnoses included foregut duplication cyst, dermoid cyst, and thyroglossal duct cyst.
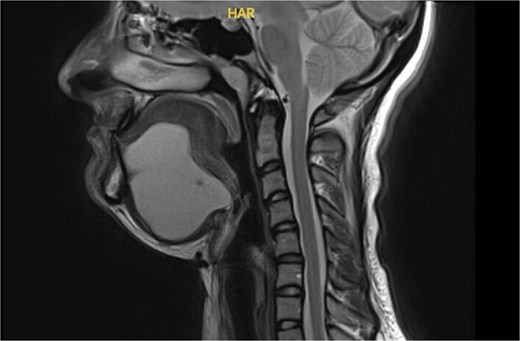
MRI neck with contrast showing a bi-lobed cystic mass extending to tongue base.
Given the size and symptomatic burden, the patient underwent excision of the mass via a midline transcervical approach. Dissection proceeded through skin and cervical fascia to the anterior bellies of the digastric muscles, which were markedly displaced and adherent to the cyst capsule. After lateral retraction of these structures, the cyst was decompressed intraoperatively to facilitate its removal, releasing a large volume of keratinous debris. The cyst was dissected free from the mylohyoid and geniohyoid muscles and the submandibular gland (Fig. 4).

Intraoperative view of dissected specimen.
Histopathology revealed a 9 × 8 cm cyst lined by orthokeratinising squamous epithelium with evidence of ulceration, granulomatous reaction, fibrosis, and cyst wall thickening—confirming a giant epidermoid cyst. No features of a foregut duplication cyst were identified. The patient remains recurrence-free at follow-up (Fig. 5).
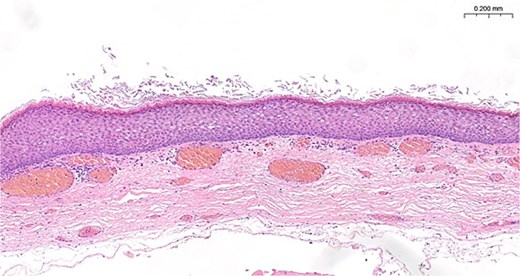
Histology showing orthokeratinizing epithelium lined cyst wall that is devoid of cutaneous appendages, the typical appearance of an epidermoid cyst.
Discussion
Dermoid cysts are benign epithelial-lined cysts that develop in areas of embryological fusion. Although only 7% of dermoid cysts occur in the head and neck region, commonly involved locations include the periorbital area, nasal dorsum, scalp, midline neck, and retroauricular region [3]. According to Meyer’s classification, these lesions are subdivided as follows:
True dermoid cysts—containing skin appendages such as hair follicles and sebaceous glands.
Epidermoid cysts—lacking skin appendages.
Teratoid cysts—containing elements from all three germ layers, including bone, muscle, vascular, respiratory, or gastrointestinal tissue [4].
A review by King et al. [5] found that floor-of-mouth cysts occur more commonly in males, with 72.9% being dermoid, 22.2% epidermoid, and 4.9% teratoid.
Dermoid and epidermoid cysts may be congenital—arising between the 3rd and 5th weeks of gestation from trapped ectodermal elements—or acquired through traumatic implantation. They enlarge slowly due to accumulated keratin or sebaceous material. In the floor of the mouth, cysts are classified relative to the mylohyoid muscle: sublingual if superior, submental if inferior. Extension through the mylohyoid, as in this case, is rare. Large cysts may cause dysphagia, dysphonia, dyspnea, and substantial cosmetic deformity.
Foregut duplication cysts differ significantly: they are true duplications of the primitive foregut, lined by respiratory or gastrointestinal mucosa and surrounded by smooth muscle. They constitute one-third of all duplication cysts, most commonly affecting the mediastinum and esophagus [6]. They are typically identified in early childhood or antenatally. Proposed embryological mechanisms include abnormal notochord separation, disordered recanalization, or persistence of embryonic diverticula [7]. In the head and neck, they may present with stridor, dysphagia, or cough, and may cause ulceration if gastric mucosa is present. Surgical excision remains the treatment of choice.
This case highlights the importance of combining clinical assessment with multimodal imaging for accurate preoperative evaluation. While ultrasound provides initial confirmation of a cystic lesion and facilitates FNA, MRI is superior in defining the extent, internal characteristics, and anatomical relationships. A cyst is considered ‘giant’ when exceeding 5 cm or demonstrating deep soft-tissue extension and significant mass effect—all of which were present in this case.
Surgical excision remains the definitive treatment for midline floor-of-mouth cysts. Sublingual cysts may be removed intraorally, whereas larger submental or trans-mylohyoid lesions often require an extraoral approach. A combined approach may be necessary in recurrent or infected lesions with scarring.
This case describes an exceptionally large epidermoid cyst of the floor of the mouth mimicking a foregut duplication cyst on imaging. Thorough clinical and radiological evaluation combined with complete surgical excision enables accurate diagnosis and effective treatment. Awareness of the potential for epidermoid cysts to extend through the mylohyoid and simulate alternative pathologies is essential for appropriate management.
Acknowledgements
We thank the patient and clinical team for consenting to the documentation and publication of this rare presentation.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}