





Abstract
Granular cell tumour (GCT) is a rare soft tissue neoplasm originally thought to arise from skeletal muscle but later recognized as of neural origin. It is most commonly found in the skin, subcutaneous tissue, and oral cavity. GCT typically presents as a painless, slow-growing nodule, often asymptomatic, though malignant cases tend to be larger and may present with pain. We present the case of a 48-year-old female that developed a painless subcutaneous swelling in the right axilla, initially suspected to be a sebaceous cyst. In November 2023, the lesion was excised, and histopathology confirmed a diagnosis of granular cell tumor. This case underscores the necessity for precise histological diagnosis in managing atypical cutaneous and subcutaneous neoplasms like GCT. A multidisciplinary approach, including regular follow-up and advanced diagnostic methods, is key to optimal management and prevention of recurrence or malignant transformation.
Introduction
Granular cell tumour (GCT), also known as granular neuroma, was first described by Abrikossoff in 1926 [1]. It is a rare soft tissue neoplasm, originally thought to be of skeletal muscle origin and termed granular cell myoblastomas [2, 3]. However, later studies using immunohistochemical techniques and electron microscopy confirmed its nervous system origin, although a subset of S100-negative GCT (non-neural) has also been identified [4].
GCT can develop anywhere in the body, including the breast, bladder, nervous system, and the aerodigestive and genitourinary tracts. However, it is most commonly found in the skin and subcutaneous tissue (30% of cases), as well as the oral cavity [5, 6]. The tumour can affect all age groups and genders, but it is more commonly seen in women aged 40 to 60, with a female-to-male ratio ranging from 1.8 to 2.4 [7–9].
GCT typically present as a single, skin-colored or brown-red, painless nodule, which is slow-growing and < 3–4 cm in diameter. While malignant tumors tend to be larger, they are rarely painful or pruritic. In 10%–15% of cases, multiple lesions may occur in the same organ or at different sites. Several studies have associated the presence of multiple GCTs with certain syndromes, such as Noonan syndrome, Neurofibromatosis type I, and Leopard syndrome [10–12].
Biologically, GCT is generally considered a benign neoplasm, with malignancy occurring in <1%–2% of cases (0.2% of all soft tissue sarcomas) [13, 14]. At present, there is no established standard treatment for GCT, with the only recommended therapy being wide local excision with negative margins to minimize the risk of recurrence. Clinical follow-up is essential for both benign and malignant cases. When excision is complete, the recurrence rate is reported to be as low as 2%–8%, but this rate increases to 21%–50% if the excision is incomplete.
For lesions suspected of being malignant, sentinel lymph node biopsy is generally recommended based on clinical evaluation or confirmed histologically. Lymph node dissection is advised for palpable lymph nodes or biopsy-proven metastatic disease [15]. Benign GCTs typically have excellent outcomes following wide local excision, with minimal recurrence or metastasis. However, patients with large, malignant lesions or metastatic disease tend to have poorer outcomes, with 5- and 10-year survival rates of 74% and 65%, respectively [5].
Surgical complications are rare but may include pain, local bleeding, bruising, surgical site infections, allergic reactions to medications, local invasion, tissue destruction, discomfort from the mass effect, metastasis (regional or distant), unsatisfactory aesthetic outcomes from scars, and recurrence [5].
Case report
We present the case of a 48-year-old female patient with a medical history of hypothyroidism, treated with levothyroxine, and fibrocystic mastopathy, which is under ongoing follow-up. In 2021, the patient developed a subcutaneous swelling in the right axillary region. Initially, it was asymptomatic and showed no signs of inflammation. During the same year, two ultrasound scans of the axillary area were performed. Both scans revealed a hypoechoic lesion with regular borders, without signs of lymph node involvement, and the initial diagnosis was a sebaceous cyst (Figs 1 and 2).
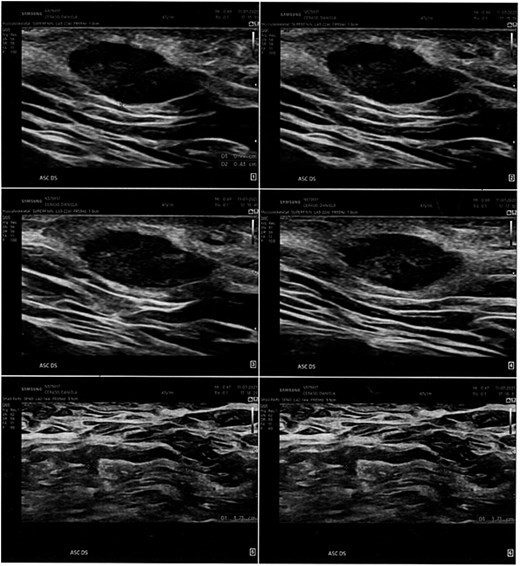
Ultrasonographic examination performed in the right axillary cavity shows in the superficial planes a centimetric oval, hypoechogenic, regular-edged shape to be varably referred to sebaceous cyst. Loco-regional lymph nodes in the deep planes, diam max 17 mm.
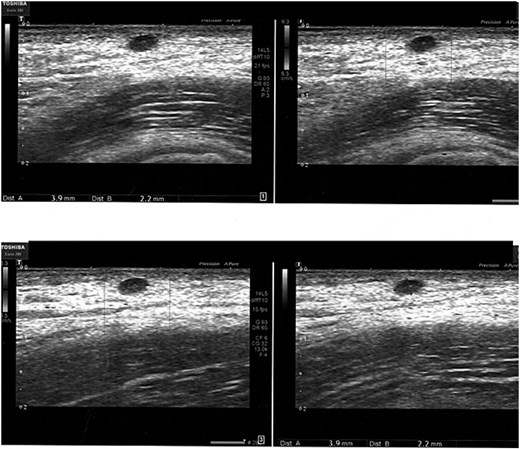
The clinically appreciable formation in the right axillary site corispondes to a todouble, well-defined contour, hypoechogenic image, lacking colorimetric signal, compatible for sebaceous cyst of 3 x 2 mm diam. Absence of locoregional lymph node hyperplasia.
Results
In 2023, the patient began experiencing increased local discomfort, with symptoms worsening around her menstrual cycle. A follow-up ultrasound in July 2023 showed no significant changes compared to the previous exams.
In November 2023, the patient sought treatment at our unit for the excision of the lesion. Histological analysis revealed a proliferation of cells with uniform nuclei and granular eosinophilic cytoplasm, without nuclear atypia or mitotic figures. Immunohistochemical testing was positive for S100, CD68, and TFE3, confirming the diagnosis of a GCT.
In December 2023, an additional surgical procedure was performed to widen the surgical margins, which showed no residual disease. One year later, the patient had fully recovered from surgery, with no signs of local recurrence.
However, in February 2025, a new skin lesion appeared on the same limb, raising suspicion of dermatofibrosarcoma. The lesion is currently under further diagnostic evaluation.
Discussion
This case underscores the importance of meticulous postoperative monitoring in managing atypical cutaneous and subcutaneous neoplasms. While GCTs are generally benign, their clinical presentation can mimic other lesions, such as sebaceous cysts, making accurate histological diagnosis essential for timely and appropriate treatment [5]. This highlights the need for thorough clinical and diagnostic evaluation, even when initial ultrasound findings suggest a benign lesion.
Although rare and typically benign, GCTs have a recurrence risk ranging from 2% to 8% following complete resection. However, in cases of incomplete excision, the recurrence rate rises significantly, reaching 21% to 50% [13]. Therefore, achieving complete resection with wide surgical margins is crucial to preventing local recurrence. In this case, margin enlargement confirmed the absence of residual disease, but annual follow-up remained essential for detecting new lesions and ensuring long-term patient monitoring.
Conclusion
This case reinforces the necessity of diligent, long-term postoperative surveillance, particularly for atypical cutaneous and subcutaneous tumors that present diagnostic challenges and carry a potential risk of recurrence or malignant transformation. A multidisciplinary approach, incorporating regular follow-up and advanced diagnostic techniques, is vital to optimizing patient management and preventing long-term complications.
Conflicts of interest
We have no conflict of interest to declare.
Funding
No funding to declare.
Informed consent
Informed consent was acquired from the patient for the publication of this case report.
Ethical statement
Our local Ethic Commitee exempt the report from approval.

{kind=link}
{kind=link}