





Abstract
Dentigerous cysts are the second most common odontogenic cysts and are frequently associated with impacted mandibular third molars. Although enucleation remains the standard treatment, regenerative approaches using autologous biomaterials have emerged as promising alternatives. This report describes the management of a mandibular dentigerous cyst in a 43-year-old female using conservative enucleation, autologous tooth-derived graft, and fibrin-rich plasma. Radiographic follow-up demonstrated early bone formation, and histopathology confirmed the diagnosis. The combined use of autologous tooth grafting and platelet concentrates represents a viable regenerative option that supports bone preservation and future rehabilitation.
Introduction
Dentigerous cysts account for ~20%–24% of odontogenic cysts and develop from fluid accumulation between the reduced enamel epithelium and the crown of an unerupted tooth [1, 2]. They most commonly involve mandibular third molars and are usually asymptomatic, being detected incidentally on radiographs. Progressive enlargement, however, may result in cortical expansion, tooth displacement, root resorption, or pathological fracture [3]. Radiographically, these lesions present as well-defined unilocular radiolucencies surrounding the crown of an impacted tooth, requiring differentiation from other odontogenic entities such as unicystic ameloblastoma or odontogenic keratocyst [3].
Conventional treatment consists of enucleation with extraction of the associated tooth. While effective, this approach may leave significant osseous defects, particularly in large mandibular lesions, potentially compromising future prosthetic or implant planning [1]. Consequently, regenerative strategies have been explored to enhance bone healing. Autologous biomaterials, including platelet-rich plasma and tooth-derived grafts, have demonstrated favorable biological properties. Tooth-derived grafts share structural and chemical similarities with bone, providing osteoconductive and osteoinductive potential, while platelet concentrates supply growth factors that enhance angiogenesis and tissue healing [4, 5].
Case presentation
A 43-year-old female with no significant medical history was referred following the incidental radiographic detection of a unilocular radiolucent lesion in the left mandibular angle associated with a horizontally impacted third molar. Clinical examination revealed no pain, inflammation, or neurosensory alterations. Panoramic imaging (Fig. 1A) and cone-beam computed tomography demonstrated a well-defined lesion at the cemento-enamel junction, with cortical thinning, buccolingual expansion, inferior alveolar canal displacement, and root resorption of adjacent molars (Fig. 1B). The differential diagnosis included unicystic ameloblastoma and odontogenic keratocyst.
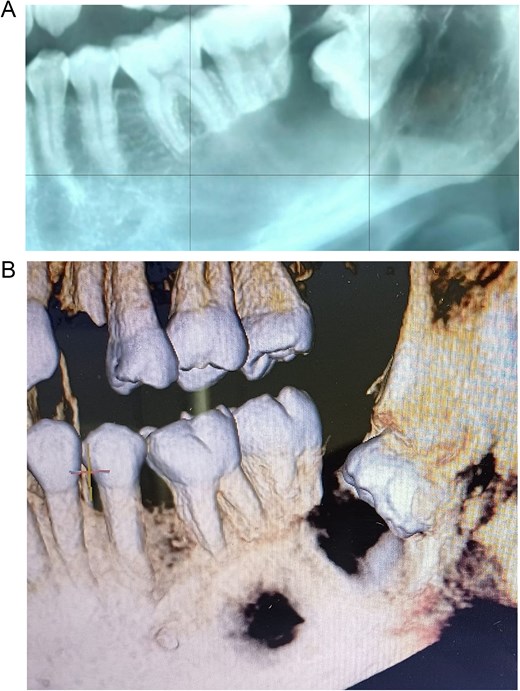
Preoperative imaging studies. (A) Panoramic radiograph. (B) Cone beam computed tomography.
Conservative surgical management was performed under general anesthesia, consisting of lesion enucleation with excisional biopsy, extraction of the impacted molar and adjacent compromised tooth (Fig. 2A–H), and reconstruction of the defect using pulverized autologous tooth graft (Fig. 2F and 3) combined with fibrin-rich plasma (Figs 2G and 4). Postoperative healing was favorable, with transient swelling, trismus, and paresthesia, which were managed with laser therapy and resolved during follow-up. Six-week radiographic evaluation demonstrated early bone formation and stability of the remaining molar (Fig. 5). Histopathological analysis confirmed a dentigerous cyst lined by non-keratinized stratified squamous epithelium with a fibrous connective tissue capsule and mild chronic inflammation (Fig. 6A and B).
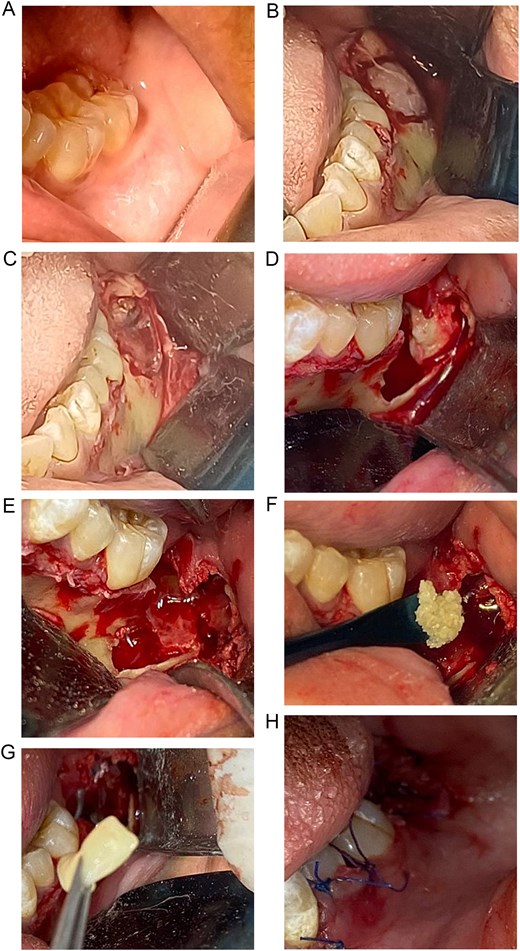
Surgical approach to the dentigerous cyst and reconstruction of the osseous defect. (A) Initial view of the posterior mandibular region at the site of the lesion. (B) Exposure of the surgical area after elevation of a mucoperiosteal flap. (C) Visualization of the cystic cavity associated with the impacted molar. (D) Removal of the cystic lesion along with extraction of the impacted molar and the compromised adjacent tooth. (E) View of the residual bone defect. (F) Compaction of the pulverized autologous tooth graft within the defect. (G) Placement of fibrin-rich plasma over the bone graft. (H) Closure of the surgical site.

KometaBio as a tooth grinder.

Platelet-rich plasma.

Postoperative radiographic control.
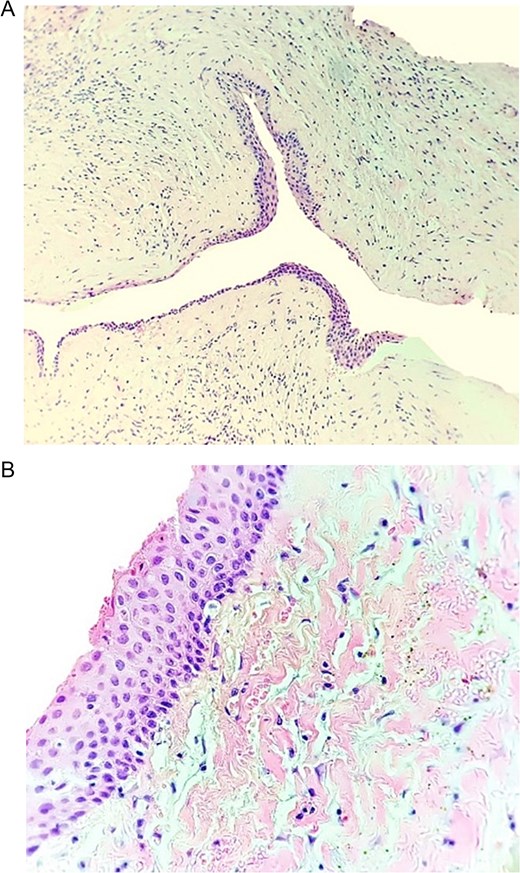
(A) Low-power view showing the cystic cavity with its fibrous capsule and the epithelial lining. Occasional inflammatory cells are present in the subepithelial connective tissue. (B) Higher magnification highlighting the epithelial lining, which is non-keratinized stratified squamous epithelium ~6–8 cell layers thick.
The patient remains under clinical and radiographic follow-up, with planned endodontic treatment of tooth 36 and subsequent assessment of bone regeneration for future implant placement.
Discussion
Early diagnosis of odontogenic cysts is essential for determining prognosis and guiding appropriate treatment, as these lesions may cause progressive bone resorption, cortical thinning, and displacement of adjacent anatomical structures if left untreated. As cysts enlarge, they compromise alveolar bone volume and may lead to functional and esthetic complications that may complicate rehabilitation. Therefore, early intervention is critical to minimizing morbidity and preserving bone integrity.
Surgical enucleation remains the standard treatment for most odontogenic cysts, allowing complete lesion removal and histopathological confirmation [1]. However, enucleation often results in residual bone defects, particularly in large lesions, where spontaneous regeneration may be delayed or incomplete. In such cases, bone regeneration procedures are necessary to restore anatomical continuity, enhance healing, and facilitate future prosthetic or implant rehabilitation [6].
Conventional bone regeneration techniques have relied on autogenous, allogenic, or xenogenic grafts. Although these materials demonstrate predictable osteoconductive properties, each presents limitations such as donor site morbidity, limited availability, or potential immunological risks [7]. These drawbacks have driven the search for alternative biomaterials with improved safety and regenerative performance.
Autologous biomaterials have gained increasing interest in regenerative dentistry [8]. Among these, tooth-derived grafts and platelet concentrates represent promising options. Extracted teeth can be processed into particulate grafts rich in hydroxyapatite, type I collagen, non-collagenous proteins, and growth factors, closely resembling the composition of natural bone and providing both osteoconductive and osteoinductive properties [4, 5, 8]. Demineralized dentin matrix has been shown to act as a scaffold capable of releasing bioactive molecules such as bone morphogenetic proteins, transforming growth factor-beta, and insulin-like growth factor, which play key roles in bone remodeling [6, 8]. Clinical and histological studies have demonstrated gradual substitution of dentin grafts by new bone within ~24 weeks, with intimate contact between graft particles and newly formed bone, indicating active remodeling [8–10].
Platelet concentrates, including platelet-rich plasma and platelet-rich fibrin, have been widely studied for their regenerative potential [11]. While several studies report enhanced soft tissue healing and angiogenesis, evidence regarding their isolated effect on bone regeneration remains inconsistent [12, 13]. Nevertheless, other investigations have demonstrated improved osseointegration and bone formation when PRP is used in combination with implants or graft materials, suggesting that its regenerative efficacy is context-dependent [14–17].
The favorable outcome observed in the present case supports existing evidence on the effectiveness of autologous tooth-derived grafts following cyst enucleation. Their biocompatibility, availability, cost-effectiveness, and ability to mimic bone structure make them a reliable regenerative option. Combined with platelet concentrates, these biomaterials align with contemporary biologically driven regenerative strategies aimed at stimulating the patient’s intrinsic healing potential. Although current evidence is promising, long-term randomized clinical trials are required to further validate their predictability and long-term stability [8].
Conclusion
Conservative enucleation of a mandibular dentigerous cyst combined with autologous tooth grafting and fibrin-rich plasma resulted in favorable clinical and radiographic outcomes, including early bone regeneration and preservation of mandibular structure. This case supports the use of autologous biomaterials as a safe, cost-effective, and biologically compatible strategy for managing osseous defects following cyst removal. Long-term studies are warranted to further validate the predictability and stability of this regenerative approach.
Author contributions
Escoto-Vasquez Lilibeth-Stephania: Writing—review and editing, Writing—original draft preparation, Visualization, Validation, Supervision, Resources, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. José Romero-Lecanda José Antonio: Visualization, Validation, Supervision, Resources, Methodology, Investigation, Formal analysis. Lomelí-Martínez Sarah Monserrat: Writing—review and editing, Writing—original draft preparation, Visualization, Validation, Supervision, Methodology, Formal analysis, Conceptualization. Martínez-Nieto Melissa: Writing—review and editing, Writing—original draft preparation, Visualization, Validation, Supervision, Methodology, Formal analysis, Conceptualization. Heboyan Artak: Writing—review and editing, Writing—original draft preparation, Visualization, Validation, Supervision, Software, Resources, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. Alarcón-Sánchez Mario Alberto: Writing—review and editing, Writing—original draft preparation, Visualization, Validation, Supervision, Software, Resources, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization.
Competing interests
All authors report no relevant conflicts of interest for this article.
Funding
None declared.
Data availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethical approval
Not applicable.
Patient informed consent
The study participant provided informed written consent prior to study enrollment.
CARE checklist (2016) statement
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}