





Abstract
We present a case of necrotising amoebic colitis (NAC) from a low-risk demographic in Sydney, Australia. A 75-year-old Caucasian male presented critically unwell with an acute abdomen and sepsis following 4 weeks of constipation and progressive abdominal pain. Computed tomography showed pneumoperitoneum, diffuse right-sided colonic wall thickening with multiple hypodense hepatic lesions. With a working diagnosis of perforated right-sided colonic cancer with liver metastases, the patient underwent an open extended right hemicolectomy. Subsequent histopathology demonstrated amoebiasis in the resected specimen. Despite active treatment, the patient died due to septic shock. As NAC is uncommon in Australia, it is often not considered as a differential diagnosis in the acute abdomen. More common diagnoses such as perforated colorectal cancer are often considered instead. Early recognition and initiation of anti-amoebic therapy, along with complete surgical resection of the affected bowel, are associated with improved survival outcomes.
Introduction
This case report presents a rare instance of fulminant necrotising amoebic colitis (NAC) in a patient from an Australian metropolitan suburb with minimal risk factors for amoebiasis. The rarity of this in a low-risk host and a non-endemic region highlights the importance of considering amoebiasis in the differential diagnosis of the acute abdomen and instituting appropriate therapy.
Case presentation
A 75-year-old Caucasian male presented to the Emergency Department of an Australian tertiary teaching hospital in a Sydney suburb with one week’s history of progressively severe abdominal pain and distension. This was associated with occasional hematochezia, unintentional weight loss and anorexia with reduced oral intake but no vomiting.
His past medical history included ischemic heart disease with prior coronary stenting, hypothyroidism, hypercholesterolemia, and osteoarthritis. He had no previous abdominal surgeries or known malignancy. A colonoscopy performed 3 years ago was unremarkable. He was a non-smoker, did not drink alcohol and had no known recent medication changes.
Examination at presentation revealed an unwell-appearing patient with a heart rate of 100 bpm, blood pressure 64/37 mmHg, respiratory rate 32, oxygen saturation 83% on 4 L/min nasal prongs and temperature 35.2°C. The abdomen was grossly distended and rigid with generalized tenderness and peritonism.
Investigations demonstrated severe lactic acidosis (pH 7.03; lactate 11.4), acute kidney injury, mild leukocytosis and striking elevation of CRP (330).
Non-contrast computed tomography (CT) of the abdomen demonstrated pneumoperitoneum and small volume free fluid in the pelvis and paracolic gutters, diffuse colonic wall thickening with mild stranding of the caecum, ascending and proximal transverse colon which also appeared relatively hypo-enhancing, and several irregular low-density foci within the liver, the largest in segment 7/8 measuring 83 × 47 × 30 mm (Fig. 1).
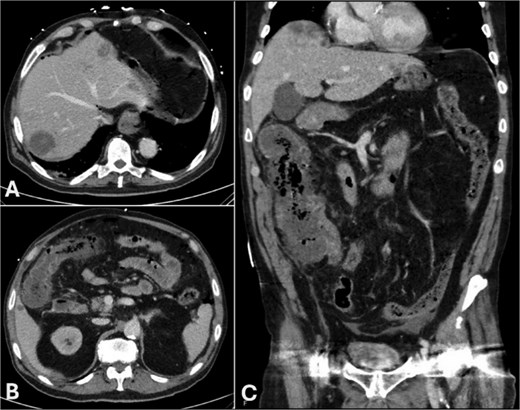
CT of the abdomen in portal venous phase: (A) subdiaphragmatic free gas and intra-hepatic hypodensities, (B) thickened hepatic flexure with hypo-enhancement, (C) thickened caecum and ascending colon with hypo-enhancement and surrounding stranding.
The patient underwent an emergency laparotomy with intraoperative findings of four-quadrant feculent peritonitis, a perforated mass at the hepatic flexure as well as a necrotic caecum with perforation into the adjacent terminal ileum and nodular deposits to the liver. The remaining transverse and descending colon were dusky appearing and were thought to be reactive inflammatory changes. Nodular deposits to the liver, and small bowel mesentery were suspicious for metastatic malignancy (Fig. 2). With a provisional diagnosis of perforated right colonic cancer with liver metastases, copious washout of the peritoneal cavity was performed, followed by an extended right hemicolectomy without anastomosis and laparostomy.

Extended right hemicolectomy specimen with perforation at the hepatic flexure (arrowhead) and caecum (arrow).
The patient was admitted to the Intensive Care Unit post-operatively for mechanical ventilation, vasopressors, hemodialysis, and broad-spectrum antibiotics.
He underwent an early relook laparotomy at 24 hours which was largely unremarkable. Another relook laparotomy at 48 hours from the index operation demonstrated healthy appearance of the terminal ileum and remaining colon. An end ileostomy and mucous fistula was formed as the patient remained in multi-organ failure.
Four days post-operation, histopathology of the resected specimen revealed NAC with ulceration, ischemia, transmural necrosis and perforation (Fig. 3). Secondary vasculitis and thrombosis was noted, along with fungal elements within necrotic tissue. Numerous amoebic trophozites were seen to be disseminated widely through the thickness of the bowel wall and within the thrombosed vessels. No malignancy was evident including all 15 lymph nodes.
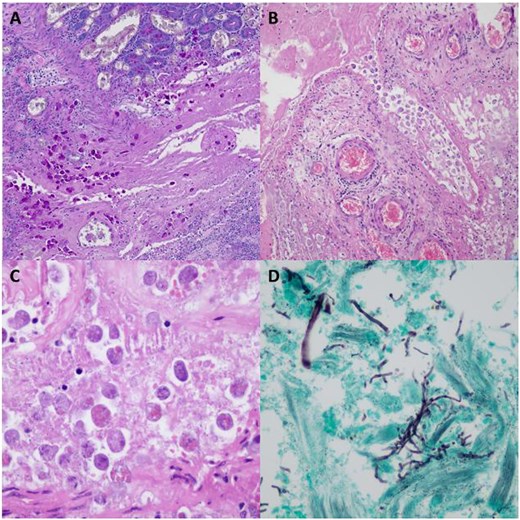
(A) 100x magnification PAS stained sections highlighting amoebic trophozoites within mucosa and submucosa of large bowel. (B) 100x magnification H&E stained section showing amoebic trophozoites within a medium sized vein in the subserosa of the large bowel. (C) 400x magnification H&E stained section showing amoebic trophozoites within an area of necrosis containing characteristic engulfed erythrocytes. (D) 400x magnification silver stain showing fungal hyphae and yeast forms.
Collateral history taken retrospectively from his family revealed that he had previously served in the Navy with likely extensive travel during this period. He retired around the age of 55 and had lived in an Australian metropolitan suburb thereafter. Further details of his prior travel and exposures could not be elicited as he remained critically unwell.
In consultation with the infectious disease team, metronidazole was commenced for treatment of amoebiasis. Repeat CT demonstrated multiple peripheral hepatic collections, the largest of which ranged from 43–125 mm in maximal dimensions, splenic collections and features of progressive enterocolitis, as well as worsening pulmonary consolidation and segmental pulmonary emboli. The hepatic collections were reviewed by interventional radiology and were deemed not amenable to percutaneous drainage. Despite reasonable efforts at directed and supportive therapy, the patient failed to improve with progressive sepsis and multi-organ failure. Following discussion with the family, he was palliated and died 11 days from admission.
Discussion
Although amoebiasis is rarely encountered in non-endemic regions like Australia, emerging data suggests that local transmission may be under-recognized. A 12-year retrospective study in Western Sydney identified multiple cases of invasive amoebiasis, with 8% having no identifiable risk factor for acquisition—implying possible local transmission [4]. In our case, the absence of traditional epidemiological risk factors such as recent travel, Indigenous background, or high-risk sexual behavior suggests a similar pattern of unexplained local acquisition.
NAC is a rare but severe complication of invasive Entamoeba histolytica infection. This affects a minority of symptomatic patients (6–11%) but carries a high fatality rate (55–100%), especially when diagnosis and treatment is delayed [3]. In a study of 30 cases, over half of the patients presented with extensive colonic necrosis and died despite surgical intervention [2]. They also found that the most common cause of death was septicemia and shock due to perforation and peritonitis [2].
The histological findings of NAC include mucosal ulceration with extensive, typically transmural inflammation and necrosis, and perforation in advanced cases. Amoebic trophozoites are typically identified at the base of ulcers within necrotic debris and appear as round organisms 10–50 μm in diameter containing characteristic intracellular erythrocytes [10].
Established risk factors for the development of NAC include male sex, advanced age, presence of amoebic liver abscesses, progressive abdominal pain, peritonitis, leukocytosis, hyponatremia, hypokalemia, and hypoalbuminemia [5]. Diabetes mellitus and other forms of immunosuppression may further contribute to disease severity [2]. Aside from immunosuppression, our patient otherwise demonstrated most of the risk factors for developing NAC.
The diagnosis of amoebiasis in Australia is challenging due to its rarity, low clinical suspicion and presentation that typically favors more common diagnoses such as colorectal malignancy, ischemic bowel or inflammatory bowel disease [1]. Conventional stool microscopy has poor sensitivity (30%–50%) but remains the gold standard [1, 2]. More recently, PCR has become more widely used due to its increased sensitivity (80%) [6]. While direct liaison with laboratories may assist with expediting results, they are often not available urgently to assist with surgical decision-making and the diagnosis is often made post-operatively as in our case [2, 4, 7].
The management of amoebic colitis involves anti-parasitic agents such as metronidazole for milder cases. Medical management alone for those with transmural involvement including perforation is insufficient and adequate surgical resection is indicated to reduce morbidity and mortality [7]. As such, the literature suggests that primary total resection of the infected colon is indicated as first line treatment in addition to anti-amoebic therapy [3, 4, 8]. He was deemed too critically unwell for a completion colectomy, so care shifted to palliation.
The Western Sydney study and other global report raise important public health considerations regarding patterns of amoebiasis infection [1, 3, 4, 9]. Increasing clinician awareness, improving diagnostic access, and including NAC in the differential for the acute abdomen could prevent delays in management. Early institution of empiric anti-parasitic therapy and timely surgical intervention may reduce the high mortality associated with this condition.
Conclusion
This case highlights the importance of considering amoebiasis and NAC in the differential diagnosis of the acute abdomen even in patients without traditional risk factors and in non-endemic regions like Australia.
Acknowledgements
The authors would like to thank Dr. Kai Zong Teo, pathologist, for providing the histology images and valuable comments on the histopathological findings.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}