





Abstract
Intra-abdominal drains are often placed during surgical procedures to prevent the formation of intra-abdominal collections and to aid early detection of leaks and hemorrhage. However, on many occasions, they can cause complications, including pain, bleeding, infection, and, on rare occasions, they can erode into the bowel, causing obstruction and even perforation. When this happens, prompt treatment is needed, as the drain can now cause severe morbidity and mortality if there is no active surveillance. Therefore, surgeons must employ an individualized approach when using drains, accounting for the specific characteristics of each surgery. We present the case of an 84-year-old patient who had a drain placed after a complicated appendicitis. After discharge, he presented with hematochezia, and after prompt evaluation, the drain was seen inside the cecum. He was successfully treated and, on follow-ups, is doing well.
Introduction
Abdominal drainage is widely used in abdominal surgery to evacuate postoperative fluid, hemorrhage, intra-operative contamination, and the risk of anastomotic failure, as well as difficulties encountered during an operation [1]. Although there are complications related to drains, perforation of the bowel is an extremely rare occurrence, with few cases ever reported in the literature [1, 2].
We present the case of a patient in whom a drain was placed after a complicated appendicitis. After discharge, he presented with hematochezia, and after prompt evaluation, the drain was seen inside the cecum.
Case report
Patient is an 84-year-old male with a past medical history of type 2 diabetes and hypertension. He presented with a 2-day history of lower abdominal pain, fever, and vomiting. At first, the pain was mild, but as time passed, it became unbearable, so he was brought in to the emergency room by his family.
On clinical evaluation, a tachycardic febrile patient with lower right abdominal tenderness was encountered. Supplementary exams revealed leukocytosis with an elevated C-reactive protein, and a computed tomography (CT) confirmed acute appendicitis, which the medical team suspected.
Surgery was decided, and on laparoscopy, multiple adhesions were seen and released. Once the 6 × 1 cm necrotic appendix was dissected, the appendiceal stump was treated using two polymeric clips, and a Jackson-Pratt drain was placed. Afterwards, the procedure was completed without complications, and he was discharged after a 3-day course of broad-spectrum antibiotics.
Six days after leaving the hospital, while being completely asymptomatic, the patient suddenly experienced severe bleeding through the anus and was rushed to the emergency room. He was hypotensive and confused, but he had no pain. On clinical evaluation, a hypotensive and tachycardic patient with hematochezia was encountered. After prompt reanimation and blood transfusion (his hemoglobin level was 7 g/dl, a decrease of 4 g/dl), he was stabilized and was admitted to investigate his lower gastrointestinal bleeding. His drainage output was low and serohematic, and he had no fever, abdominal pain, or other symptoms.
A colonoscopy was planned to identify the cause of his condition, and on the ascending colon near the cecum, a white foreign body was seen covered in blood clots. After extensive washing, the Jackson-Pratt drain end was discovered perforating the cecum while the pear-shaped silicone bulb was filled with air. No other lesions, bleeding sites, or perforations were seen (Fig. 1).

Colonoscopy shows the tip of the drain within the cecum, surrounded by blood clots.
Lower gastrointestinal bleeding due to a perforation of the cecum wall, caused by drainage, was the final diagnosis.
A new contrast-enhanced CT (Fig. 2A and B) was performed, confirming that the drain was perforating the bowel without pneumoperitoneum or inflammation, and, as the patient remained asymptomatic, a conservative management of the drain perforation was decided and treated as a cecal fistula. The drain was left in place for 10 days and removed due to low and serous output (Fig. 3). The patient was discharged without complications and remained on close follow-up. One year after surgery, he is doing well.
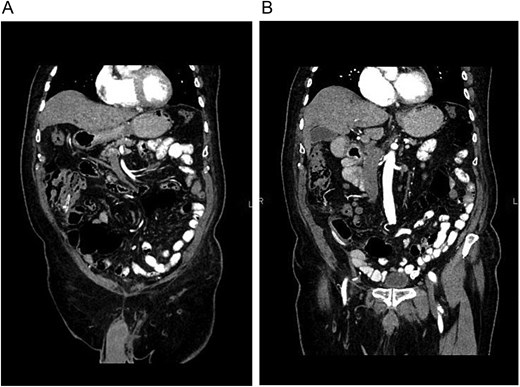
(A) CT, the drain is seen within the colon. (B) CT, no free air or fat stranding is seen around the colon or drain.

Bulb of the drain with serous output.
Discussion
Surgical drains are common in all types of surgical procedures, and one of the most common is the Jackson-Pratt drain, which was developed in 1971 by Dr Frederick E. Jackson and Dr Richard A. Pratt [1].
Drains are placed, as a general rule, in the presence of hemorrhage, intra-operative contamination, risk of anastomotic failure, and difficulties encountered during the operation [1, 3]. However, like any medical procedure, nothing is risk-free, and complications of drainage have been described, including infection, pain, hemorrhage, hernias, eviscerations, adhesions, and even bowel lesions [3].
Erosion of the drain into the bowel is an extremely rare complication, with only a few cases described in the English literature [1–4]. Although the physiopathology is not fully understood, it’s believed that the risk of erosion and perforation is caused by suction from the drain, which remains in contact with the bowel wall, causing pressure necrosis and erosion [2]. This can be explained by the fact that the side holes of a suction drain can reach a level of −180 mmHg. However, other factors should also be considered, including the drain’s flexibility and stiffness [2, 4]. In our case, our patient recently underwent an appendectomy, which could have caused an entry site for the drain, leading to perforation and bleeding.
If there are signs of peritonitis or severe hemorrhage, surgical or endoscopic procedures must be promptly completed; however, in some scenarios, if the patient is asymptomatic, it can be managed conservatively if there are no signs of perforation or obstruction and the patient can pass gas and feces [1, 4, 5]. The drain can be removed after the fifth or seventh day if its output is serous and less than 50 cc [1, 2, 6]. As prolonged maintenance periods have been associated with even more complications [3, 7].
In our case, our patient presented with lower gastrointestinal bleeding, and the drain was identified within the cecum. After adequate resuscitation and with the patient remaining asymptomatic, conservative treatment was used with excellent results.
Careful placement and vigilance of a patient a drain and during every procedure are of paramount importance. Soft-type drains should be placed, carefully monitored, and removed at the earliest safe time following the surgery.
Conflicts of interest
The authors declare no conflict of interests.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}