





Abstract
Amyand’s hernia (AH) is a rare clinical entity characterized by the presence of the appendix within an inguinal hernia sac, with or without associated appendicitis, and is rarely diagnosed preoperatively due to its nonspecific clinical presentation. We report the case of a 66-year-old woman who presented with an irreducible right inguinal swelling accompanied by severe right lower abdominal pain. Contrast-enhanced computed tomography (CT) revealed an inflamed appendix within the hernial sac, consistent with a strangulated AH. The patient underwent appendectomy along with hernia repair, with an uneventful postoperative recovery. Although acute appendicitis within an AH is typically identified intraoperatively, advances in imaging (particularly CT scanning) allow accurate preoperative diagnosis and facilitate appropriate surgical planning. Management should be tailored according to Losanoff and Basson’s classification, with appendectomy and hernia repair being an effective approach for type II AH cases.
Introduction
A hernia occurs when an organ protrudes through a weakened area in the wall of its cavity [1]. There are many types of hernias, classified based on their anatomical location: inguinal hernia, femoral hernia, umbilical hernia, incisional hernia, hiatal hernia, etc. The most frequent type of hernia is the inguinal hernia which occurs when abdominal contents protrude through a defect in the inguinal region. Consequently, inguinal hernioplasty is one of the most frequently performed surgeries worldwide [2].
Amyand’s hernia (AH) represents a rare variation of inguinal hernia characterized by the presence of the appendix within the hernial sac. It accounts for approximately 1% of all inguinal hernias [3].
In 1735, Claudius Amyand first described this unusual hernia presentation in an 11-year-old male patient. The absence of specific diagnostic signs makes preoperative identification of this condition particularly challenging, usually discovered incidentally during surgery or identified through computed tomography (CT) imaging [4, 5].
While most AH cases remain clinically silent, some patients may develop acute appendicitis and ischemic complications such as incarceration, strangulation, phlegmon formation, or perforation. These acute ischemic events remain rare, occurring at a reported frequency of 0.1% [6].
Case presentation
A 66-year-old female presented with sudden onset right lower abdominal pain. The pain was severe, continuous, colicky in nature, and radiated to the right groin. It was associated with nausea, vomiting, and anorexia but no fever, altered bowel habits, or urinary symptoms. She reported a palpable right inguinal swelling, which had recently become tender and irreducible. Her past medical history was unremarkable. Her past surgical history included total abdominal hysterectomy 20 years ago and right inguinal hernia repair 6 years ago.
On examination: The patient was conscious, alert, and oriented but irritable due to pain. Her vital signs were: Temperature: 36°C, Spo2: 96%, HR: 74 bpm, BP: 120/60 mmHg. Abdominal exam showed a tender, irreducible 5 × 6 cm right inguinal swelling with moderate tension but no skin changes. Mild suprapubic tenderness was noted. Blood tests revealed hemoglobin level (Hb) of 12.3 g/dL, white blood cell (WBC) count of 6.3 × 103/μL, and C-reactive protein (CRP) of 91.6 mg/dL. The urine analysis revealed microscopic hematuria (red blood cell count: 7 cells/high power field).
A standing abdominal X-ray showed no air-fluid levels or signs of intestinal obstruction (Fig. 1). Abdominal ultrasound revealed a right inguinal hernia with herniated fat structures, with no definitive internal vascularity and mild fluid inside, suggestive of strangulation, there was a short, blind-ended tubular structure inside the hernia of maximal thickness 7.5 mm highly suggestive of an inflamed appendix.

AP abdominal radiograph. The image reveals a non-obstructive bowel gas pattern. There is significant fecal loading of the colon, consistent with constipation or slow colonic transit. No evidence of small bowel obstruction or perforation is seen.
Contrast enhanced abdomen and pelvic CT scan revealed a right inguinal hernia containing omental fat and approximately three quarters of the appendix. The herniated appendix appeared dilated with a diameter of 1 cm, demonstrating wall edema, periappendiceal fat stranding, and adjacent fluid collection. Post-contrast images showed no enhancement of the herniated contents, consistent with vascular compromise and strangulation (Fig. 2). These findings support the diagnosis of a strangulated AH complicated by acute appendicitis and ischemic changes within the hernial sac.
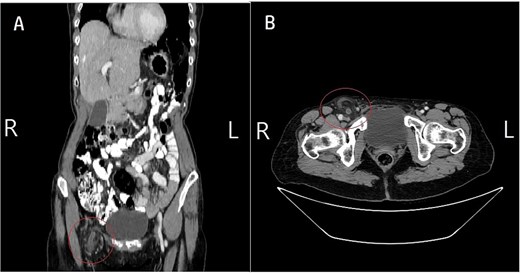
Contrast-enhanced CT scan confirming strangulated AH. (A) Axial view: CT shows the right inguinal hernia sac containing the dilated appendix (1 cm diameter). Note the significant periappendiceal fat stranding and adjacent fluid, confirming acute appendicitis. (B) Coronal view: CT clearly demonstrates the inflamed appendix and omental fat descending from the right lower quadrant and entering the right inguinal canal. The images collectively showed no enhancement of the herniated contents, consistent with vascular compromise and strangulation.
Operative procedure (appendectomy with hernia repair): The patient was classified as ASA I. Under general anesthesia and sterile conditions, a right iliac fossa gridiron incision was made. A direct hernia sac was identified, containing the appendix, which showed gangrenous changes at the tip. The mesoappendix was dissected and ligated; the appendiceal base was doubly tied, and appendectomy was completed with mucosal cauterization. The hernia sac was reduced, and the posterior wall was plicated using non-absorbable polypropylene (Prolene 1–0) sutures, followed by a modified Bassini tissue repair. Mesh repair was avoided due to the contaminated surgical field, as prosthetic material in the presence of infection increases the risk of surgical site infection and mesh-related complications. Hemostasis was achieved, and the wound was closed in layers using Vicryl sutures and skin clips. The specimen was sent for histopathology, confirming acute appendicitis with periappendicitis.
The postoperative course was uneventful. The patient resumed oral intake on the first postoperative day and was mobilized on the same day. No surgical drains were placed. She was discharged on postoperative Day 2 in stable condition and prescribed oral cefuroxime 500 mg twice daily for 7 days. She was advised to avoid heavy lifting. Follow-up at 2 weeks and 2 months showed no evidence of surgical site infection, recurrence, or other complications.
Discussion
AH has been documented across all age groups, with reported cases ranging from neonates (3 weeks) to elderly patients (88 years) [7].
Among the various pathophysiological theories for AH, the congenital hypothesis suggests that persistence of the embryological fibrous tract between the appendix and right testis, along with a patent processus vaginalis, creates an anatomical predisposition. This may explain the higher prevalence of AH in pediatric compared to adult populations [1, 8].
Anatomic anomalies predisposing to left AH formation include intestinal malrotation, situs inversus, and hypermobile cecal variants [9].
The pathophysiology of appendicitis occurring within an AH differs from conventional acute appendicitis. Unlike typical appendicitis, which results from luminal obstruction, inflammation in AH often results from mechanical factors such as vascular compromise due to hernia strangulation or direct trauma to the appendix within the constricted sac [10–12].
AH requires differentiation from various conditions including complicated inguinal hernias, acute appendicitis, urogenital emergencies, and soft tissue infections, reflecting the anatomical complexity of the inguinal region.
The definitive diagnosis of AH is typically confirmed intraoperatively but several modalities aid in preoperative suspicion. Laboratory markers such as leukocytosis and elevated CRP can be supportive, but up to 40% of patients with confirmed pathology demonstrate normal white blood cell counts and CRP levels [13]. Ultrasound imaging shows a non-compressible, blind-ended tubular structure, cecum linked tubular structure in the hernia sac, and CT scanning, which is considered the preferred method for identifying the herniated appendix and associated complications such as wall thickening, periappendiceal fat stranding, or perforation [13, 14]. MRI may be used as an alternative in pediatric or pregnant patients when ultrasound findings are inconclusive.
The management of AH depends on its classification according to Losanoff and Basson classification described in Table 1 [15].
The management of AH according to Losanoff and Basson.
| Classification | Description | Surgical management |
|---|---|---|
| Type 1 | Normal appendix within an inguinal hernia | Hernia reduction, mesh repairs, appendectomy in young patients |
| Type 2 | Acute appendicitis within hernia, no abdominal sepsis | Appendectomy through hernia primary repair of hernia, no mesh |
| Type 3 | Acute appendicitis within an inguinal hernia, abdominal wall, or peritoneal sepsis | Laparotomy, appendectomy, primary repair of hernia, no mesh |
| Type 4 | Acute appendicitis within an inguinal hernia, related or unrelated abdominal pathology | Manage as type 1 to 3 hernia investigate or treat second condition as appropriate |
Our case is type 2 AH (Acute appendicitis within hernia, no abdominal sepsis), It was managed with appendectomy and hernia repair. Intraoperatively, the posterior wall was plicated using non-absorbable polypropylene (Prolene 1–0) sutures, followed by a modified Bassini tissue repair. Although Modified Bassini’s repair is less effective than Lichtenstein method (tension-free repair), it was more convenient to be used for this patient because of the risk of post-operative infection due to the infected appendicitis.
AH may lead to several serious complications, including periappendiceal or appendicular abscess formation, appendiceal perforation with subsequent intra-abdominal abscess development, and rarely, necrotizing fasciitis of the anterior abdominal wall. Additional potential complications comprise scrotal fistula formation due to chronic inflammation. These complications typically arise from delayed diagnosis or inadequate treatment of the herniated, inflamed appendix within the inguinal canal [10].
Conclusion
The presence of the appendix within an inguinal hernia sac is referred to as AH. Appendicitis within an AH is rare. Preoperative diagnosis remains challenging. Contrast-enhanced abdominal and pelvic CT scanning is the preferred imaging modality and can enable accurate preoperative diagnosis. Although the incidence of this hernia type is rare, the appendix may become incarcerated within AH and lead to further complications such as strangulation and perforation.
Acknowledgements
The authors express their profound gratitude to the Polytechnic Medical Students’ Research Association (PMRA) for their invaluable contributions and unwavering support that significantly enriched every stage of the research journey.
Author contributions
Abed Samara and Ashwaq Khalayfeh: Conceptualization, Case analysis, Manuscript writing, and Editing.
Ashwaq Khalayfeh, Ghina Abukamleh, and Abed Samara: Data collection, Literature review, and Manuscript drafting.
Reem Sabah and Taha Z. Makhlouf: Clinical management of the patient, Data interpretation, and Manuscript revision.
All authors have read and approved the final manuscript and agree to be accountable for all aspects of the work.
Conflicts of interest
We declare that no conflict of interest could be perceived as prejudicing the impartiality of the research reported.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not for-profit sectors.
Data availability
The data used to support the findings of this study are included in the article.
Informed consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal if requested.
Ethical approval
Ethical approval was not applicable for this study, as our institution’s IRB committee does not mandate approval for reporting individual cases or case series.

{kind=link}
{kind=link}