





Abstract
Chronic calcifying pancreatitis (CCP) is rare in adolescents and is associated with significant morbidity, including chronic pain. Although endoscopic and minimally invasive techniques have expanded treatment options, surgery remains the cornerstone of management in complicated cases. The Partington–Rochelle (PR) procedure is widely used, but long-term outcomes may be suboptimal when associated complications are present. We report the case of a 15-year-old Senegalese girl presenting with chronic epigastric pain and weight loss over two years. Imaging demonstrated CCP with marked dilation of the main pancreatic duct and a large pancreatic pseudocyst. Given extensive ductal calculi, the associated pseudocyst, and limited access to advanced endoscopic therapy, surgical management was selected as first-line treatment. A modified PR procedure combined with cholecystectomy, choledochoduodenostomy, and cystogastrostomy was performed. Postoperative recovery was uneventful. A modified PR procedure combined with biliary and cystic diversion may provide durable symptom relief and favorable long-term outcomes in selected adolescents with complicated CCP.
Introduction
Chronic calcifying pancreatitis (CCP) is a rare condition in adolescents, with genetic factors accounting for the majority of cases [1–3]. The disease-related pain and complications impose a considerable burden, with negative effects on quality of life, school attendance, and recurrent hospitalizations [1, 2, 4, 5]. Despite the growing role of endoscopic techniques and lithotripsy, surgery remains the cornerstone of treatment in low-resource settings with limited endoscopic availability. Furthermore, data on the management of adolescent CCP in Africa remain scarce. Several surgical strategies have been described, including drainage procedures, pancreatic resections, and combined techniques [6, 7]. However, no consensus exists regarding a standardized surgical approach [7]. Among drainage procedures, the Partington–Rochelle (PR) procedure, consisting of a longitudinal side-to-side pancreaticojejunostomy, has been associated with low morbidity and mortality due to preservation of pancreatic parenchyma [7]. Nevertheless, failure of the PR procedure is not uncommon and may result from inadequate ductal decompression, anastomotic stenosis, unrecognized biliary obstruction, or associated pancreatic pseudocysts. Moreover, ductal decompression alone may not provide sustained pain relief, with recurrence reported in up to 50% of cases [1, 8]. This raises the question of the potential benefit of combining the PR procedure with prophylactic biliodigestive diversion, particularly in patients living in low-resource settings. We report the case of a Senegalese adolescent with CCP complicated by a pancreatic pseudocyst, successfully treated with a PR procedure combined with cholecystectomy, choledochoduodenostomy, and cystogastrostomy, resulting in favorable long-term outcomes.
Case report
A 15-year-old girl was admitted with a painful epigastric mass associated with recurrent vomiting, evolving over two years. She reported repeated episodes of refractory abdominal pain and progressive weight loss, resulting in significant disruption of school attendance. There was no family history of pancreatic disease and no history of alcohol or drug use. Physical examination revealed a fixed, mildly tender epigastric mass measuring ~7 cm. Laboratory investigations showed microcytic hypochromic anemia (hemoglobin 7.2 g/dl) and a prothrombin rate of 78.9%. Renal function, serum electrolytes, fasting blood glucose, liver function tests, tumor markers (CA 19–9 and CEA), serum calcium, and triglyceride levels were within normal limits. Computed tomography revealed pancreatic macrocalcifications, marked dilation of the Wirsung duct, and a large pancreatic pseudocyst measuring 107 × 83 × 140 mm, with minimal intraperitoneal fluid (Fig. 1). These findings were consistent with CCP complicated by a pancreatic pseudocyst. After appropriate preoperative optimization, exploratory laparotomy was performed under general anesthesia. Intraoperative findings included a fibrotic, inflamed pancreas, a large interhepatogastric pseudocyst arising from the pancreatic body, and signs of segmental portal hypertension. Needle aspiration of the pancreatic parenchyma yielded a brown-colored pancreatic juice (Fig. 2). Longitudinal pancreatotomy centered on the dilated Wirsung duct revealed multiple intraductal calculi, which were extracted, followed by ductal irrigation (Fig. 2). A side-to-side pancreaticojejunostomy using a transmesocolic Roux-en-Y limb was performed (Fig. 3). Cholecystectomy, side-to-side choledochoduodenostomy, and cystogastrostomy with cavity drainage were also carried out. The postoperative course was uneventful. Oral feeding was started on postoperative day 5. Histopathological examination confirmed chronic pancreatitis with pancreatic pseudocyst. Long-term follow-up demonstrated complete pain relief, weight gain, and resumption of normal school activities.
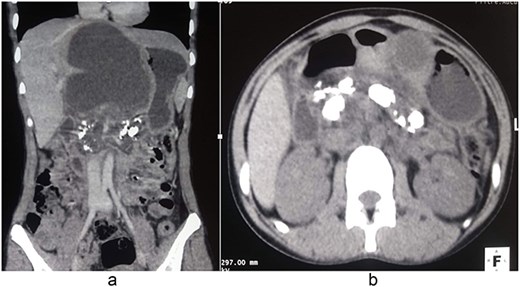
Contrast-enhanced computed tomography showing CCP complicated by a large pancreatic pseudocyst. (a) Coronal reconstruction demonstrating a large pancreatic pseudocyst with associated pancreatic duct calcifications. (b) Axial image showing extensive intraductal pancreatic calcifications consistent with CCP.
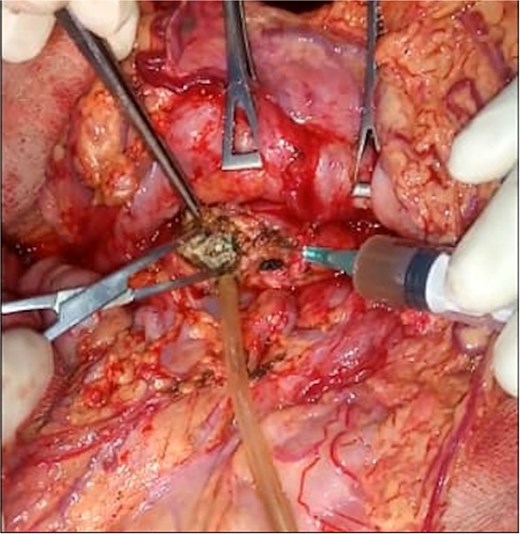
Intraoperative view demonstrating removal of intraductal pancreatic calculi (white arrow) after punction of dilated Wirsung duct and pancreatotomy.
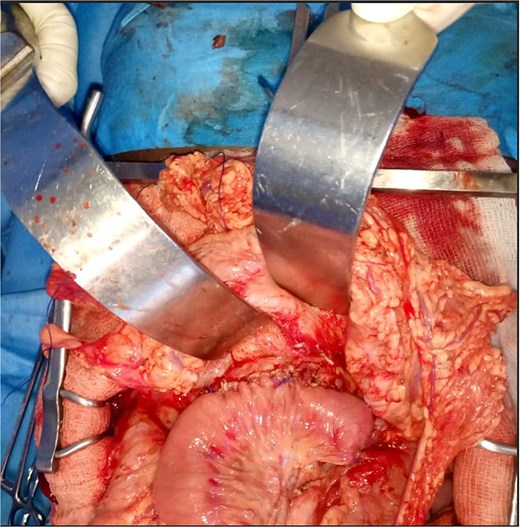
Intraoperative view showing a side-to-side pancreaticojejunostomy performed on a Roux-en-Y limb.
Discussion
In adolescent patients, CCP is a rare and debilitating condition, often refractory to conservative management. It is most commonly associated with genetic mutations (PRSS1, SPINK1, CFTR) or obstructive etiologies such as pancreatic duct anomalies or gallstones [4]. In our patient, no obstructive cause was identified on imaging, and genetic testing could not be performed due to limited resources. The goals of CCP management include durable pain relief, treatment of complications, preservation of pancreatic endocrine and exocrine function, and improvement of quality of life [1]. Surgery is indicated when conservative treatment fails, although it may be considered as first-line therapy in patients with extensive ductal calculi, significant ductal dilation, or associated complications [3, 6, 9]. Various surgical procedures exist for the management of chronic pancreatitis, including drainage, resections, and a combination of partial resections and drainage [6, 7]. Drainage procedures, particularly the PR technique, are preferred in patients with a dilated pancreatic duct, as extensive resections increase the risk of pancreatic insufficiency [5]. Our patient presented with marked dilation of the Wirsung duct without inflammatory enlargement of the pancreatic head, making her an ideal candidate for the PR procedure. Surgery was chosen as first-line treatment due to the extensive calcifications, large pseudocyst, and absence of endoscopic therapeutic options in our setting. We performed a PR procedure combined with cholecystectomy, choledochoduodenostomy, and cystogastrostomy. The biliodigestive bypass was intended to prevent biliary stenosis and reflux-related complications, while cystogastrostomy addressed the pancreatic pseudocyst. The large pancreatic duct diameter reduced the risk of postoperative pancreatic fistula, which did not occur in our patient. Resection procedures are generally indicated for patients without ductal dilation (diameter ˂ 3 mm) or with inflammatory head masses, while combined drainage–resection techniques are indicated when ductal dilation is associated with pancreatic head hypertrophy [10]. In CCP without dilation of the Wirsung duct (<5 mm), or in cases of a narrow pancreatic duct, the Izbicki procedure is recommended [10]. This technique combines pancreatic drainage and limited resection by creating a V-shaped groove on the anterior surface of the pancreas, which serves as the drainage channel [10]. While the PR procedure yields encouraging short-term results, some studies with extended long-term follow-up have demonstrated diminishing efficacy, with recurrence of persistent symptoms reported up to 15 years after the initial surgery [1, 7]. Our patient had an uneventful postoperative course, with favorable long-term outcomes. At 5 years of follow-up, she remained asymptomatic, without evidence of exocrine or endocrine pancreatic insufficiency. These results corroborate previously published data demonstrating the safety and efficacy of the PR procedure with low morbidity and mortality. Importantly, the addition of biliodigestive diversion in this case proved highly effective in preventing the development of biliary strictures.
Conclusion
CCP in adolescents is a rare and complex condition with significant functional and metabolic implications. No standardized surgical strategy currently exists. This case highlights the relevance and effectiveness of combining biliary and cystic diversion with the PR procedure in selected patients. This conservative and prophylactic surgical approach appears particularly suitable for young patients, especially in low-resource settings, given its favorable long-term outcomes.
Authors contribution
All authors contributed to the management of the patient. Dr. Mohamadou Lamine Gueye drafted the present manuscript, which was reviewed and approved by all co-authors.
Conflicts of interest
There is no conflict of interest.
Funding
This study received no specific funding.
Consent for publication
Written informed consent was obtained from the patient’s legal guardian for publication of this case report and any accompanying images.

{kind=link}
{kind=link}
{kind=link}