





Abstract
Coronary artery fistulas (CAFs) are rare vascular malformations that can result in catastrophic outcomes for patients. The development of CAFs is often accompanied by significant dilation and/or aneurysmal changes in the supplying coronary artery. Management of CAFs depends on the symptomatic status. We report a 52-year-old woman who presented to our hospital with unexplained chest tightness and pain for 2 weeks. Definitive diagnosis of a right CAF with aneurysmal dilation was established through comprehensive evaluation. The patient underwent surgical intervention involving incision at the proximal posterior atrioventricular groove coronary aneurysm, with successful fistula ligation via continuous suture closure. CAF are rare, often clinically silent anomalies of significant pathophysiologic importance, with a risk of lethal complications. This case demonstrates the feasibility and technical considerations of open surgical repair for a giant saccular coronary aneurysm secondary to fistula. It underscores the importance of an individualized surgical strategy in managing such complex anatomy.
Introduction
Coronary artery fistulas (CAFs) are rare diseases that occur in 0.002% of the general population and account for 0.1% of coronary anomalies [1]. The formation of CAFs is often accompanied by marked dilation and/or aneurysmal changes in the supplying artery, primarily due to increased blood flow caused by the fistula itself, which can lead to the development of giant aneurysms [2]. CAFs most commonly originate from the right coronary artery and drain into the right ventricle, while drainage into the right atrium is uncommon [3]. Because of its rarity and frequently asymptomatic nature, the diagnosis is often challenging. Echocardiography alone may not detect the CAFs, requiring integration of physical examination, ECG findings, imaging, and comprehensive clinical judgment for diagnosis [4]. Management of CAFs with aneurysmal coronary arteries is determined by the presence of clinical manifestations. Asymptomatic cases may be treated conservatively with pharmacotherapy, whereas surgical intervention is indicated for symptomatic patients to prevent potential complications such as artery rupture, myocardial ischemia, and thrombus formation. Established surgical techniques include ligation, patch repair and bypass graft, arterial incision and suture reconstruction, etc. [5, 6]. This report describes a rare symptomatic right coronary artery-to-right atrium fistula in a 52-year-old woman, who underwent indicated surgical repair.
Case presentation
A 52-year-old woman presented to our hospital with a 2-week history of idiopathic chest tightness and chest pain. Physical examination showed systolic hypertension (140/73 mmHg). The patient had no personal or family history of cardiovascular risk factors, such as hypertension, hyperlipidemia, or diabetes mellitus. The electrocardiogram obtained at admission showed a heart rate of 80 beats per minute, normal sinus rhythm, and T-wave abnormalities. Initial laboratory evaluation revealed elevated B-type natriuretic peptide levels, while serum troponin T remained within normal limits. Routine transthoracic echocardiography revealed aneurysmal coronary artery dilation with abnormal flow trajectory (Fig. 1). Parasternal long-axis views demonstrated aneurysmal dilation of the right coronary sinus and proximal right coronary artery (Fig. 1A). Subsequent apical five-chamber views identified a fistulous orifice in the right coronary artery draining superior to the tricuspid septal leaflet into the right atrium (Fig. 1B), with a measured orifice diameter of ~5.8 mm. Subsequent coronary computed tomography angiography (CCTA) with three-dimensional reconstruction confirmed our echocardiographic findings, revealing extensive aneurysmal dilation of the right coronary artery with an RCA – RA fistula (Fig. 2A–D, Supplementary Video 1). Selective coronary angiography was performed during hospitalization, which further confirmed the presence of a giant right coronary artery aneurysm (Fig. 2E and F, Supplementary Video 2) and revealed no significant stenosis or pathology in the left coronary system. Furthermore, cardiac catheterization quantified a pulmonary-to-systemic flow ratio (Qp:Qs) of 1.8:1, indicating a moderate left-to-right shunt. Based on these findings, the patient was diagnosed with a right CAF and a giant right coronary artery aneurysm.

Transthoracic echocardiogram. (A) The parasternal long-axis view demonstrates aneurysmal dilation of the right coronary artery, with the proximal segment dilated to ~9 mm in diameter. Color Doppler echocardiography demonstrates turbulent flow within the dilated coronary artery segment(arrow). (B) The apical five-chamber view demonstrates the right atrium and right ventricle under color Doppler echocardiography. Color Doppler echocardiography reveals turbulent flow originating superior to the tricuspid septal leaflet, oriented toward the right atrium, with an associated perforation measuring ~5.8 mm in diameter (arrow).
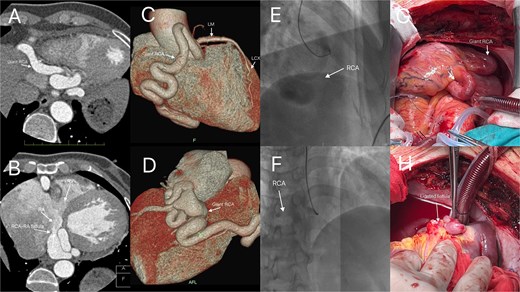
Enhanced CT coronary angiography confirmed the presence of a right coronary artery to right atrium fistula with a giant right coronary artery (A, B, arrows). Three-dimensional reconstruction (C, D, arrows) and selective coronary angiography further confirmed these findings (E, F, arrows). Intraoperative photograph clearly showing the giant right coronary artery (G, arrow), and the patient subsequently underwent fistula ligation under cardiopulmonary bypass (H, arrow).
Given the patient’s significant chest discomfort and pain, along with clear surgical indications and no contraindications, fistula ligation was performed via median sternotomy on cardiopulmonary bypass. Following cannulation of the aorta, superior vena cava, and inferior vena cava, the lines were de-aired and connected to the cardiopulmonary bypass circuit. The patient was systemically cooled to a nasopharyngeal temperature of 32°C. Given the significant coronary steal phenomenon, meticulous myocardial protection was paramount. Our strategy consisted of antegrade cold blood cardioplegia administered via the aortic root, supplemented by topical cardiac cooling with ice-slush saline. Particular attention was paid to the infusion pressure and volume of the cardioplegic solution due to the potential for altered distribution caused by the fistula. Complete electromechanical arrest of the heart was subsequently confirmed. During the procedure, a right atriotomy was performed and the coronary sinus orifice was enlarged, but no distinct fistula was identified. Attempts to locate it by administering antegrade cardioplegia via the aortic root yielded no visible reflux. Consequently, the coronary artery aneurysm in the proximal posterior atrioventricular groove was incised, revealing the fistula (~6 mm in diameter) within the aneurysm lumen. The fistula was then repaired using 5-0 pledgeted sutures in an interrupted followed by a continuous fashion (Fig. 2G and H). After verifying fistula closure and performing coronary aneurysmorrhaphy, the right atriotomy was repaired using 4-0 polypropylene. The caval snares were released, the heart was de-aired, and the aortic cross-clamp was removed, resulting in the spontaneous return of sinus rhythm. The total aortic cross-clamp time was 55 min. The patient was rewarmed to 36.8°C. Cardiopulmonary bypass was discontinued after 67 min of total support, the cannulas were removed, and meticulous hemostasis was achieved.
Following surgery, the patient was transferred to the intensive care unit (ICU) for further management. Upon ICU admission, the patient received continuous vasoactive agent infusion for blood pressure support, dexamethasone for edema reduction, protamine for heparin reversal, and cefazolin sodium (1 g) for antibiotic prophylaxis. Her postoperative course was stable, with transfer from the ICU on the following day. Follow-up CCTA showed no significant abnormalities (Fig. 3A and B). The patient was discharged on postoperative day 7. Upon discharge, the patient was prescribed a single antiplatelet regimen of aspirin (100 mg daily) to prevent thrombosis at the coronary arteriotomy and aneurysm repair sites, with careful consideration of bleeding risks. This medication plan was intended for adjustment according to subsequent imaging surveillance. Follow-up during the first postoperative year included scheduled CCTA and echocardiography every 3 months, alongside regular clinical visits.
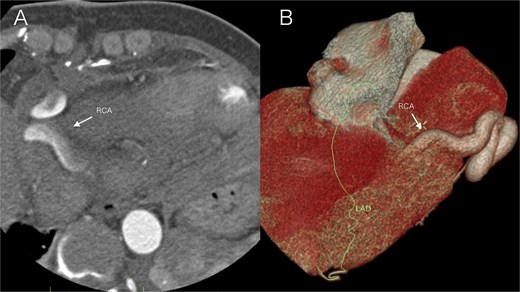
Postoperative imaging on day 5 after surgical repair of a right coronary artery fistula with giant aneurysm. (A) Axial contrast-enhanced CT image at the level of the aortic root. The right coronary artery (arrow) demonstrates a normalized caliber and wall contour, with complete resolution of the preoperative aneurysmal dilation. (B) Volume-rendered three-dimensional CT reconstruction (anterolateral view). The reconstruction focuses on the course of the right coronary artery (arrow), which exhibits a smooth, uniform, and patent lumen without evidence of the previous aneurysm or fistula.
Discussion
CAFs represent rare vascular anomalies, predominantly congenital in origin, while a smaller subset results from iatrogenic trauma. These anomalies result from abnormal connections between coronary arteries and major vessels (arterial or venous) or cardiac chambers. The chronic high-flow shunt through these communications can lead to progressive dilation or even aneurysmal formation in the feeding coronary artery. These anomalies result from abnormal connections between coronary arteries and major vessels (arterial or venous) or cardiac chambers. CAFs are typically asymptomatic during childhood, with clinical manifestations usually emerging in adulthood after age 18. Common presentations include angina pectoris, arrhythmias, and heart failure. Potential complications encompass coronary artery dilation, mural thrombus formation, and coronary aneurysm rupture [7].
Diagnosis of CAFs relies on physical examination, electrocardiography (ECG), and advanced imaging modalities. Physical examination may reveal a continuous precordial murmur. ECG findings are typically normal but can demonstrate volume overload patterns, including increased R-wave amplitude, suggesting left ventricular hypertrophy. Coronary angiography remains the gold standard for diagnosing CAFs, while echocardiography, CCTA, and three-dimensional coronary reconstruction serve as complementary diagnostic modalities [8]. These techniques provide critical visualization of coronary morphology, along with detailed characterization of fistula size, configuration, and shunt volume—essential for guiding subsequent therapeutic strategies.
This report presents a case of a symptomatic patient with a CAF and associated aneurysmal dilation. The patient’s symptoms of chest pain and tightness indicated the coronary steal phenomenon; subsequent definitive evaluation with echocardiography, CCTA, and angiography confirmed the indication for surgical intervention.
The management of CAFs with aneurysmal dilation depends on symptom presence. Asymptomatic patients typically receive conservative treatment, including antiplatelet therapy and regular surveillance [9]. For symptomatic cases, intervention remains the definitive approach, primarily categorized as either interventional operation or open surgical repair, with modality selection depending on fistula anatomy and complexity.
Interventional surgery is indicated in patients whose anatomy is favorable for the procedure, including those with a single narrow drainage site, a proximal fistula origin, an absence of multiple fistulas or large branch vessels, and/or an absence of concomitant cardiac disorders [10]. Surgical approaches, employed for complex cases, include ligation, patch repair, bypass grafting, internal closure of the fistula, Arterial incision and suture reconstruction, etc. [11]. This patient presented with a CAF complicated by aneurysmal dilation, constituting a complex case. Of note, in patients with CAFs demonstrating significant shunt flow and coronary steal, the initiation of cardiopulmonary bypass poses a specific risk of ventricular fibrillation secondary to an abrupt alteration in coronary perfusion pressure. Key preventive and management strategies include: (i) the preoperative placement of defibrillation pads; (ii) maintaining an elevated systemic perfusion pressure during the initial phase of bypass; and (iii) preparedness for immediate electrical cardioversion should fibrillation occur, followed by rapid aortic cross-clamping and administration of cardioplegic solution. In the present case, fistula ligation was successfully accomplished under cardiopulmonary bypass. This procedure effectively mitigates the long-term risks of aneurysm rupture and thrombotic complications. Following surgery, the patient experienced significant alleviation of preoperative chest pain and was enrolled in a structured long-term surveillance program.
Conclusions
In conclusion, we report a rare case of a CAF with a giant right coronary artery aneurysm. The patient underwent meticulous diagnosis and surgical repair, achieving an uneventful postoperative recovery. Given that coronary fistulas are frequently asymptomatic or minimally symptomatic yet carry a substantial risk of serious complications, establishing precise diagnostic criteria and selecting optimal management strategies are paramount, underscoring the necessity for further research into this uncommon pathology.
Author contributions
Y.H.L. and L.L.L. contributed to data collection and analysis. Y.H.L. wrote this article. F.X.Y. support and encouraged the study. All authors read and approved the final manuscript.
Conflicts of interest
None declared.
Funding
The study did not receive any funding.
Data availability
No datasets were generated or analyzed during the current study.
Consent for publication
Consent was obtained from the patient for the publication of this report.

{kind=link}
{kind=link}
{kind=link}